

One-unit versus two-unit cord-blood transplantation for hematologic cancers
- PMID: 25354103
- PMCID: PMC4257059
- DOI: 10.1056/NEJMoa1405584
One-unit versus two-unit cord-blood transplantation for hematologic cancers
Abstract
Background: Umbilical-cord blood has been used as the source of hematopoietic stem cells in an estimated 30,000 transplants. The limited number of hematopoietic cells in a single cord-blood unit prevents its use in recipients with larger body mass and results in delayed hematopoietic recovery and higher mortality. Therefore, we hypothesized that the greater numbers of hematopoietic cells in two units of cord blood would be associated with improved outcomes after transplantation.
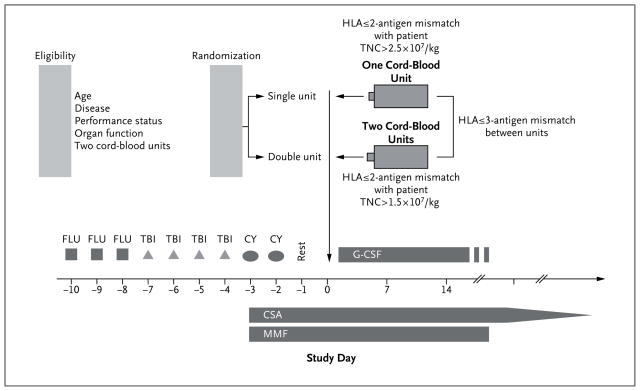
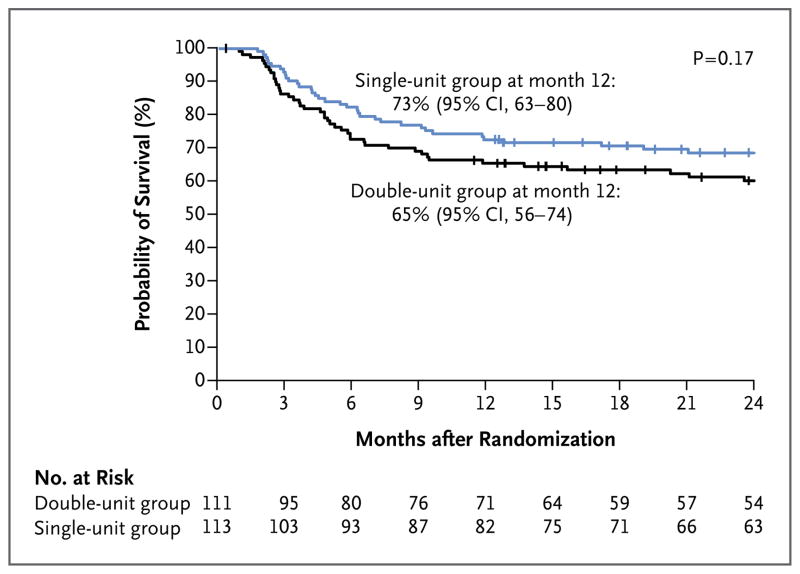
Methods: Between December 1, 2006, and February 24, 2012, a total of 224 patients 1 to 21 years of age with hematologic cancer were randomly assigned to undergo double-unit (111 patients) or single-unit (113 patients) cord-blood transplantation after a uniform myeloablative conditioning regimen and immunoprophylaxis for graft-versus-host disease (GVHD). The primary end point was 1-year overall survival.
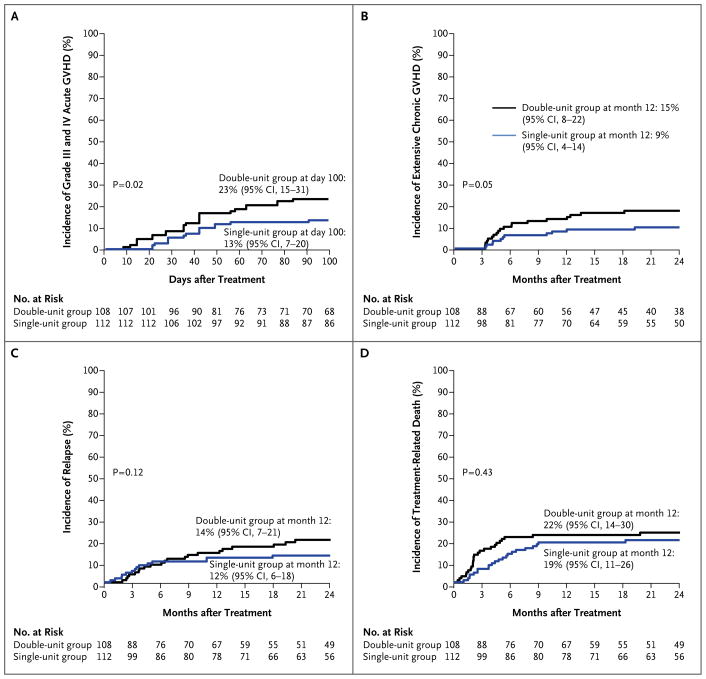
Results: Treatment groups were matched for age, sex, self-reported race (white vs. nonwhite), performance status, degree of donor-recipient HLA matching, and disease type and status at transplantation. The 1-year overall survival rate was 65% (95% confidence interval [CI], 56 to 74) and 73% (95% CI, 63 to 80) among recipients of double and single cord-blood units, respectively (P=0.17). Similar outcomes in the two groups were also observed with respect to the rates of disease-free survival, neutrophil recovery, transplantation-related death, relapse, infections, immunologic reconstitution, and grade II-IV acute GVHD. However, improved platelet recovery and lower incidences of grade III and IV acute and extensive chronic GVHD were observed among recipients of a single cord-blood unit.
Conclusions: We found that among children and adolescents with hematologic cancer, survival rates were similar after single-unit and double-unit cord-blood transplantation; however, a single-unit cord-blood transplant was associated with better platelet recovery and a lower risk of GVHD. (Funded by the National Heart, Lung, and Blood Institute and the National Cancer Institute; ClinicalTrials.gov number, NCT00412360.).
Figures
Comment in
-
One-unit versus two-unit cord-blood transplantation.N Engl J Med. 2015 Jan 15;372(3):288. doi: 10.1056/NEJMc1414419. N Engl J Med. 2015. PMID: 25587953 No abstract available.
-
One-unit versus two-unit cord-blood transplantation.N Engl J Med. 2015 Jan 15;372(3):287. doi: 10.1056/NEJMc1414419. N Engl J Med. 2015. PMID: 25587954 No abstract available.
-
One-unit versus two-unit cord-blood transplantation.N Engl J Med. 2015 Jan 15;372(3):287-8. doi: 10.1056/NEJMc1414419. N Engl J Med. 2015. PMID: 25587955 No abstract available.
References
-
- Rubinstein P, Carrier C, Scaradavou A, et al. Outcomes among 562 recipients of placental-blood transplants from unrelated donors. N Engl J Med. 1998;339:1565–77. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 HL069294/HL/NHLBI NIH HHS/United States
- U10-HL069294/HL/NHLBI NIH HHS/United States
- U24 CA076518/CA/NCI NIH HHS/United States
- U10 HL069249/HL/NHLBI NIH HHS/United States
- UG1 HL069274/HL/NHLBI NIH HHS/United States
- U10 CA098543/CA/NCI NIH HHS/United States
- U10 HL069246/HL/NHLBI NIH HHS/United States
- U10 CA180886/CA/NCI NIH HHS/United States
- U01 HL069246/HL/NHLBI NIH HHS/United States
- P30 CA077598/CA/NCI NIH HHS/United States
- U10CA098543/CA/NCI NIH HHS/United States
- U10 HL069290/HL/NHLBI NIH HHS/United States
- U10 HL069274/HL/NHLBI NIH HHS/United States
- P01 CA065493/CA/NCI NIH HHS/United States
- P01CA065493-21/CA/NCI NIH HHS/United States
- U10 HL069330/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials