

Is Hepatic Resection for Large or Multifocal Intrahepatic Cholangiocarcinoma Justified? Results from a Multi-Institutional Collaboration
- PMID: 25354576
- PMCID: PMC4834710
- DOI: 10.1245/s10434-014-4223-3
Is Hepatic Resection for Large or Multifocal Intrahepatic Cholangiocarcinoma Justified? Results from a Multi-Institutional Collaboration
Abstract
Background: The role of surgical resection for patients with large or multifocal intrahepatic cholangiocarcinoma (ICC) remains unclear. This study evaluated the long-term outcome of patients who underwent hepatic resection for large (≥7 cm) or multifocal (≥2) ICC.
Methods: Between 1990 and 2013, 557 patients who underwent liver resection for ICC were identified from a multi-institutional database. Clinicopathologic characteristics, operative details, and long-term survival data were evaluated.
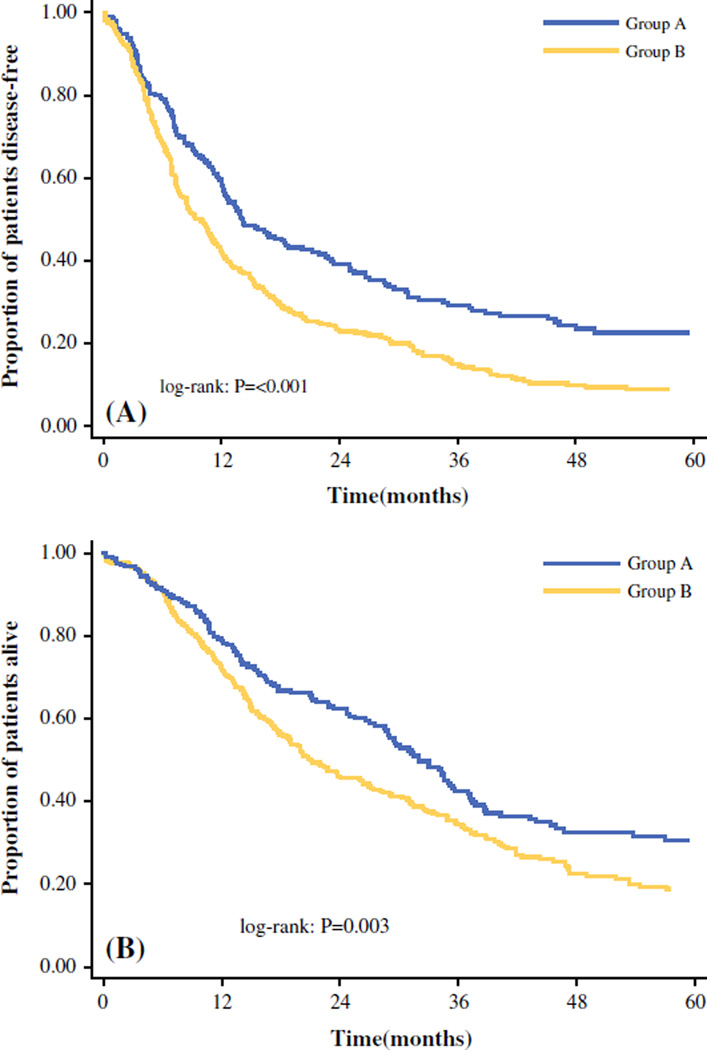
Results: Of the 557 patients, 215 (38.6 %) had a small, solitary ICC (group A) and 342 (61.4 %) had a large or multifocal ICC (group B). The patients in group B underwent an extended hepatectomy more frequently (16.9 vs. 30.4 %; P < 0.001). At the final pathology exam, the patients in group B were more likely to show evidence of vascular invasion (22.5 vs. 38.5 %), direct invasion of contiguous organs (6.5 vs. 12.9 %), and nodal metastasis (13.3 vs. 21.0 %) (all P < 0.05). Interestingly, the incidences of postoperative complications (39.3 vs. 46.8 %) and hospital mortality (1.1 vs. 3.7 %) were similar between the two groups (both P > 0.05). The group A patients had better rates for 5-year overall survival (OS) (30.5 vs. 18.7 %; P < 0.05) and disease-free survival (DFS) (22.6 vs. 8.2 %; P < 0.05) than the group B patients. For the patients in group B, the factors associated with a worse OS included more than three tumor nodules [hazard ratio (HR), 1.56], nodal metastasis (HR, 1.47), and poor differentiation (HR, 1.48).
Conclusions: Liver resection can be performed safely for patients with large or multifocal ICC. The long-term outcome for these patients can be stratified on the basis of a prognostic score that includes tumor number, nodal metastasis, and poor differentiation.
Conflict of interest statement
Figures

References
-
- Bektas H, Schrem H, Kleine M, et al. Primary liver tumours: presentation, diagnosis and surgical treatment. InTech. 2013:91–116.
-
- Aljiffry M, Abdulelah A, Walsh M, Peltekian K, Alwayn I, Molinari M. Evidence-based approach to cholangiocarcinoma: a systematic review of the current literature. J Am Coll Surg. 2009;208:134–147. - PubMed
-
- Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology. 2001;33:1353–1357. - PubMed
-
- Shaib YH, Davila JA, McGlynn K, El-Serag HB. Rising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase? J Hepatol. 2004;40:472–477. - PubMed
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24:115–125. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
