

Mechanochemical endovenous ablation versus radiofrequency ablation in the treatment of primary small saphenous vein insufficiency (MESSI trial): study protocol for a randomized controlled trial
- PMID: 25354769
- PMCID: PMC4228073
- DOI: 10.1186/1745-6215-15-421
Mechanochemical endovenous ablation versus radiofrequency ablation in the treatment of primary small saphenous vein insufficiency (MESSI trial): study protocol for a randomized controlled trial
Abstract
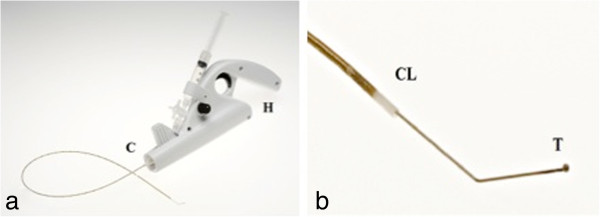
Background: Minimally invasive endothermal techniques, for example, radiofrequency ablation (RFA), have revolutionized the treatment of insufficient truncal veins and are associated with an excellent outcome. The use of thermal energy requires the instillation of tumescent anesthesia around the vein. Mechanochemical endovenous ablation (MOCA™) combines mechanical endothelial damage, using a rotating wire, with simultaneous infusion of a liquid sclerosans. Tumescent anesthesia is not required as no heat is used. Prospective studies using MOCA™ in both great and small saphenous veins showed good anatomical and clinical results with fast postoperative recovery.
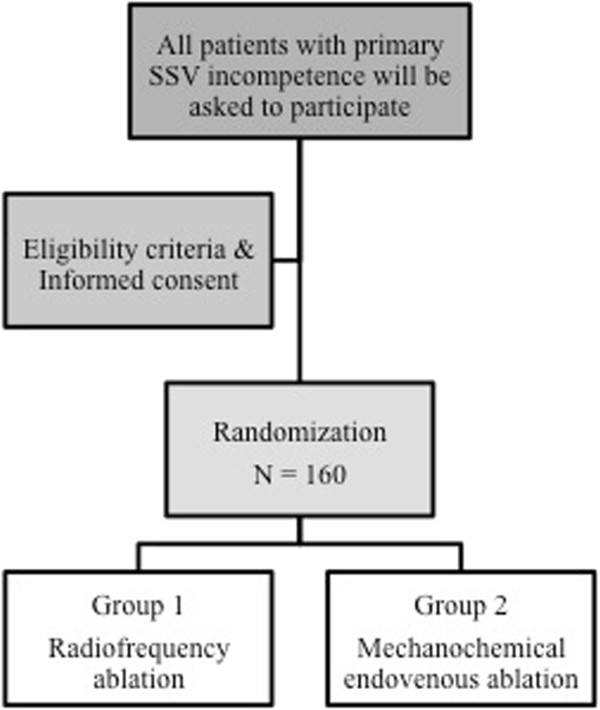
Methods/design: The MESSI trial (Mechanochemical Endovenous ablation versus radiofrequency ablation in the treatment of primary Small Saphenous vein Insufficiency) is a multicenter randomized controlled trial in which a total of 160 patients will be randomized (1:1) to MOCA™ or RFA. Consecutive patients with primary small saphenous vein incompetence, who meet the eligibility criteria, will be invited to participate in this trial. The primary endpoint is anatomic success, defined as occlusion of the treated veins objectified with duplex ultrasonography at 1 year follow-up. Secondary endpoints are post-procedural pain, initial technical success, clinical success, complications and the duration of the procedure. Initial technical success is defined as the ability to position the device adequately, treat the veins as planned and occlude the treated vein directly after the procedure has been proven by duplex ultrasonography. Clinical success is defined as an objective improvement of clinical outcome after treatment, measured with the Venous Clinical Severity Score (VCSS). Power analyses are conducted for anatomical success and post-procedural pain.Both groups will be evaluated on an intention-to-treat principle.
Discussion: The hypothesis of the MESSI trial is that the anatomic success rate of MOCA™ is not inferior to RFA. The second hypothesis is that post-procedural pain is significantly less after MOCA compared to RFA.
Trial registration: NTR4613 Date of trial registration: 28 May 2014.
Figures
References
-
- Andreozzi GM, Cordova RM, Scomparin A, Martini R, D’Eri A, Andreozzi F. Quality of life working group on vascular medicine of SIAPAV. Quality of life in chronic venous insufficiency. An Italian pilot study of the Triveneto Region. Int Angiol. 2005;24:272–277. - PubMed
-
- Almgren B, Eriksson E. Valvular incompetence in superficial, deep and perforator veins of limbs with varicose veins. Acta Chir Scand. 1990;156:69–74. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
