

Outcomes of a partnered facilitation strategy to implement primary care-mental health
- PMID: 25355087
- PMCID: PMC4239280
- DOI: 10.1007/s11606-014-3027-2
Outcomes of a partnered facilitation strategy to implement primary care-mental health
Abstract
Background: Implementing new programs and practices is challenging, even when they are mandated. Implementation Facilitation (IF) strategies that focus on partnering with sites show promise for addressing these challenges.
Objective: Our aim was to evaluate the effectiveness of an external/internal IF strategy within the context of a Department of Veterans Affairs (VA) mandate of Primary Care-Mental Health Integration (PC-MHI).
Design: This was a quasi-experimental, Hybrid Type III study. Generalized estimating equations assessed differences across sites.
Participants: Patients and providers at seven VA primary care clinics receiving the IF intervention and national support and seven matched comparison clinics receiving national support only participated in the study.
Intervention: We used a highly partnered IF strategy incorporating evidence-based implementation interventions.
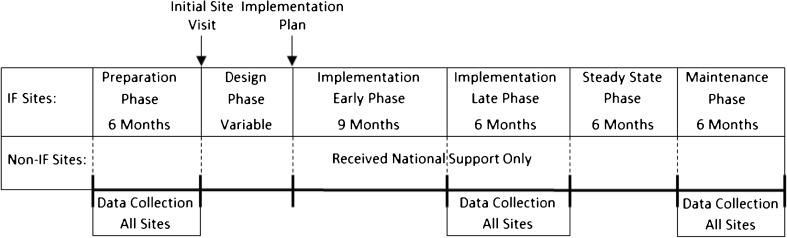
Main measures: We evaluated the IF strategy using VA administrative data and RE-AIM framework measures for two 6-month periods.
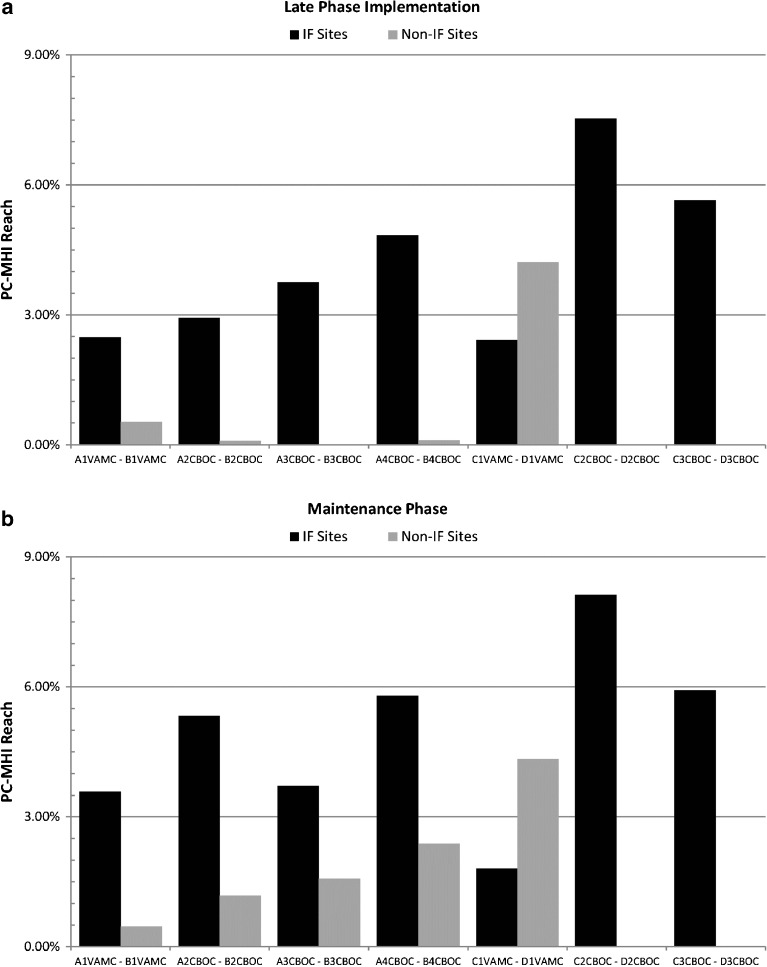
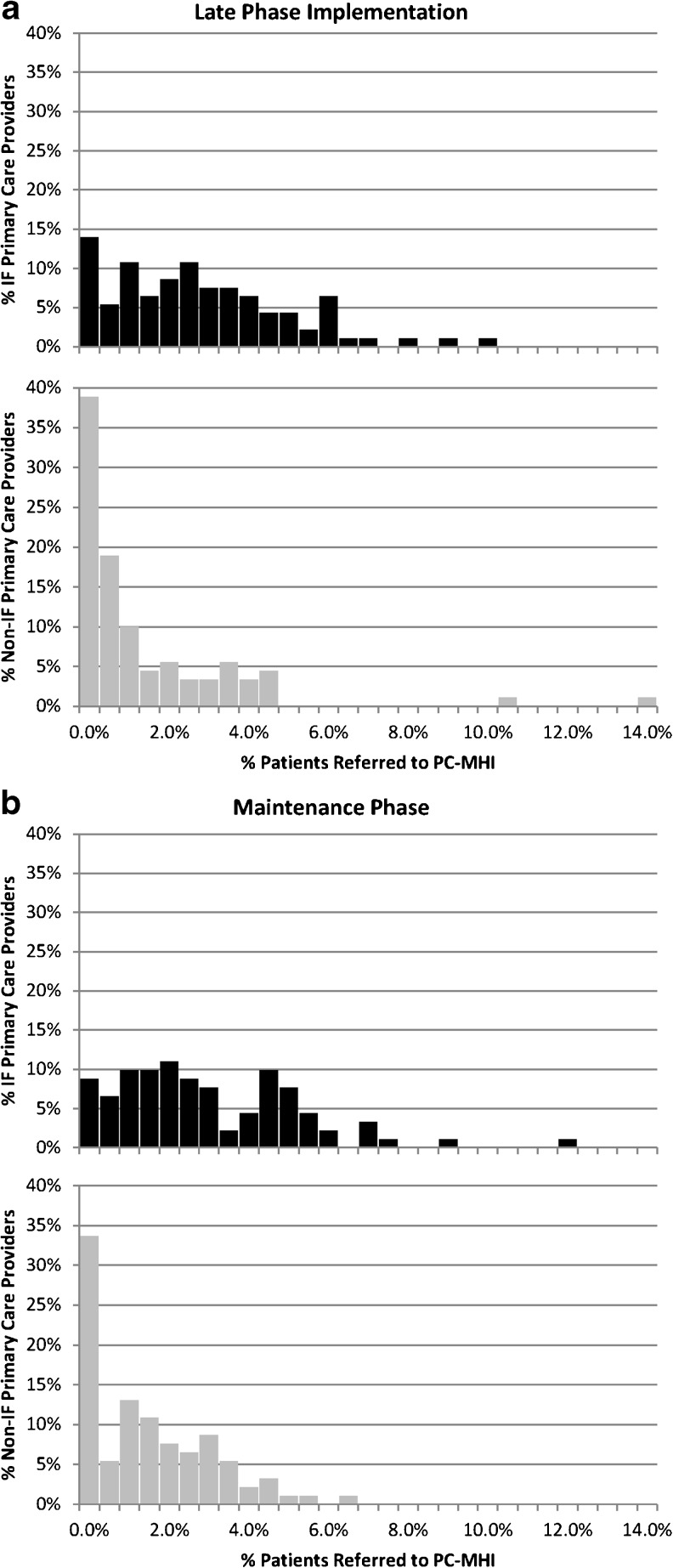
Key results: Evaluation of RE-AIM measures from the first 6-month period indicated that PC patients at IF clinics had nine times the odds (OR=8.93, p<0.001) of also being seen in PC-MHI (Reach) compared to patients at non-IF clinics. PC providers at IF clinics had seven times the odds (OR=7.12, p=0.029) of referring patients to PC-MHI (Adoption) than providers at non-IF clinics, and a greater proportion of providers' patients at IF clinics were referred to PC-MHI (Adoption) compared to non-IF clinics (β=0.027, p<0.001). Compared to PC patients at non-IF sites, patients at IF clinics did not have lower odds (OR=1.34, p=0.232) of being referred for first-time mental health specialty clinic visits (Effectiveness), or higher odds (OR=1.90, p=0.350) of receiving same-day access (Implementation). Assessment of program sustainability (Maintenance) was conducted by repeating this analysis for a second 6-month time period. Maintenance analyses results were similar to the earlier period.
Conclusion: The addition of a highly partnered IF strategy to national level support resulted in greater Reach and Adoption of the mandated PC-MHI initiative, thereby increasing patient access to VA mental health care.
Figures
Similar articles
-
Using implementation facilitation to foster clinical practice quality and adherence to evidence in challenged settings: a qualitative study.BMC Health Serv Res. 2017 Apr 20;17(1):294. doi: 10.1186/s12913-017-2217-0. BMC Health Serv Res. 2017. PMID: 28424052 Free PMC article.
-
Changing Patterns of Mental Health Care Use: The Role of Integrated Mental Health Services in Veteran Affairs Primary Care.J Am Board Fam Med. 2018 Jan-Feb;31(1):38-48. doi: 10.3122/jabfm.2018.01.170157. J Am Board Fam Med. 2018. PMID: 29330238
-
Using implementation facilitation to implement primary care mental health integration via clinical video telehealth in rural clinics: protocol for a hybrid type 2 cluster randomized stepped-wedge design.Implement Sci. 2019 Mar 21;14(1):33. doi: 10.1186/s13012-019-0875-5. Implement Sci. 2019. PMID: 30898129 Free PMC article.
-
Evaluating mental health care and policy in Spain.J Ment Health Policy Econ. 2010 Jun;13(2):73-86. J Ment Health Policy Econ. 2010. PMID: 20919594 Review.
-
Evidence-based psychosocial treatment in the community: considerations for dissemination and implementation.Psychooncology. 2016 May;25(5):482-90. doi: 10.1002/pon.3864. Epub 2015 Jun 17. Psychooncology. 2016. PMID: 27092813 Free PMC article. Review.
Cited by
-
Correlates of Emergency Department Use by Individuals With Bipolar Disorder Enrolled in a Collaborative Care Implementation Study.Psychiatr Serv. 2016 Nov 1;67(11):1265-1268. doi: 10.1176/appi.ps.201500347. Epub 2016 Jun 1. Psychiatr Serv. 2016. PMID: 27247174 Free PMC article. Clinical Trial.
-
Evaluation of implementation facilitation integrated into a national mentoring programme to improve access to evidence-based psychotherapy for post-traumatic stress disorder within the veterans health administration: a quality improvement report.BMJ Open Qual. 2024 Jan 12;13(1):e002449. doi: 10.1136/bmjoq-2023-002449. BMJ Open Qual. 2024. PMID: 38216294 Free PMC article.
-
Key components of external facilitation in an acute stroke quality improvement collaborative in the Veterans Health Administration.Implement Sci. 2015 May 14;10:69. doi: 10.1186/s13012-015-0252-y. Implement Sci. 2015. PMID: 25971405 Free PMC article.
-
Getting a clinical innovation into practice: An introduction to implementation strategies.Psychiatry Res. 2020 Jan;283:112467. doi: 10.1016/j.psychres.2019.06.042. Epub 2019 Jul 2. Psychiatry Res. 2020. PMID: 31488332 Free PMC article. Review.
-
What can implementation science offer civil society in their efforts to drive rights-based health reform?Glob Health Res Policy. 2023 Jan 17;8(1):1. doi: 10.1186/s41256-023-00284-4. Glob Health Res Policy. 2023. PMID: 36650592 Free PMC article.
References
-
- National Research Council . Improving the quality of health care for mental and substance-use conditions: Quality Chasm Series. Washington, DC: The National Academies Press; 2006. - PubMed
-
- Grol R, Wensing M, Eccles M. Improving Patient Care: The Implementation of Change in Clinical Practice. London: Elsevier; 2005.
-
- Wensing M, Fluit C, Grol R. Educational Strategies. In: Grol R, Wensing M, Eccles M, Davis D, editors. Improving Patient Care: The Implementation of Change in Clinical Practice. 2. West Sussex, UK: John Wiley and Sons, Ltd.; 2013. pp. 197–209.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
