

Oxygen kinetics during 6-minute walk tests in patients with cardiovascular and pulmonary disease
- PMID: 25355483
- PMCID: PMC4223731
- DOI: 10.1186/1471-2466-14-167
Oxygen kinetics during 6-minute walk tests in patients with cardiovascular and pulmonary disease
Abstract
Background: The 6-Minute Walk Test (6MWT) is representative of daily-life activities and reflects the functional capacity of patients. The change of oxygen uptake (VO2) in the initial phase of low-intensity exercise (VO2 kinetics) can be used to assess submaximal exercise performance of patients.The objective of the following study was to analyse VO2 kinetics in patients with different pulmonary and cardiovascular diseases. In addition, we investigated the extent to which VO2 kinetics at the onset of the 6MWT were associated with exercise capacity, morbidity and mortality.
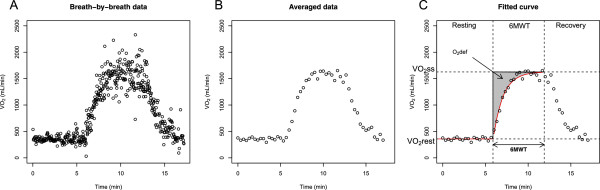
Methods: VO2 kinetics of 204 patients and 16 healthy controls were obtained using mobile telemetric cardiopulmonary monitoring during a 6MWT. A new mean response time (MRT) index (wMRT) was developed to quantify VO2 kinetics by correcting MRT for work rate. The differences in wMRT between disease categories as well as the association between wMRT and patients' exercise capacity and outcome - time to hospitalization/death- were tested.
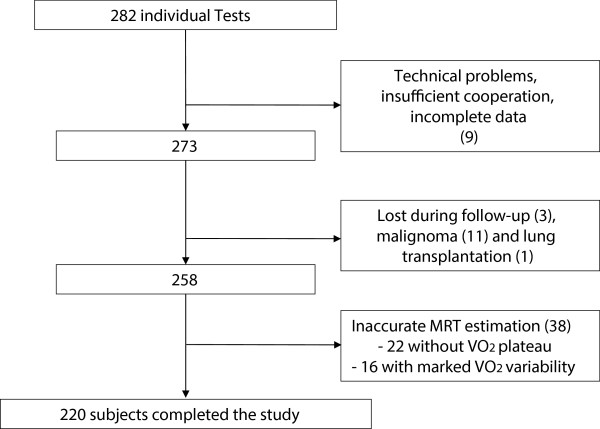
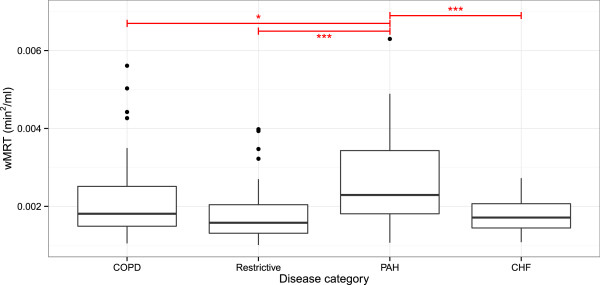
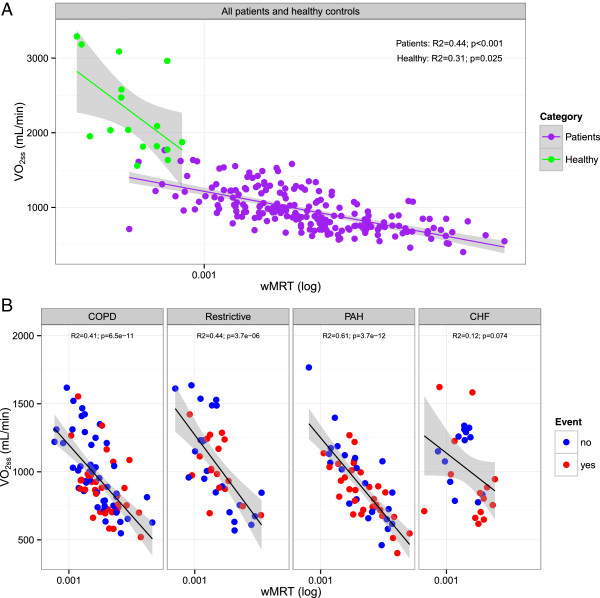
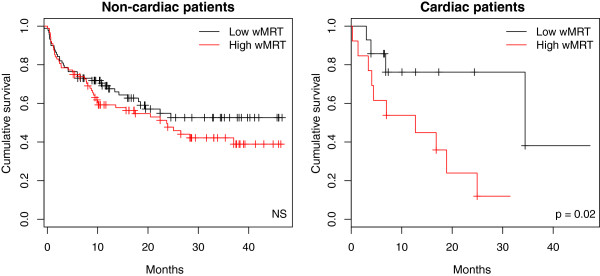
Results: The assessment of a robust wMRT was feasible in 86% (244/284) patients. wMRT was increased in patients compared to healthy controls (p <0.001). wMRT was largest in patients with pulmonary arterial hypertension (PAH). There were significant associations between wMRT and exercise capacity in all patients. High wMRT was found to be associated with a high rate of death and re-hospitalization in patients with CHF (p = 0.024). In patients with pulmonary diseases and pulmonary hypertension wMRT was not associated with outcome (p = 0.952).
Conclusions: Submaximal exercise performance of patients is reduced. O2 kinetics at the onset of exercise are associated with exercise capacity in all patients. wMRT was found to be an important prognostic factor in patients with congestive heart failure (CHF), but not with pulmonary diseases.
Figures
Similar articles
-
Cardiopulmonary and gas-exchange responses during the six-minute walk test in patients with chronic obstructive pulmonary disease.Respiration. 2014;88(4):307-14. doi: 10.1159/000365997. Epub 2014 Sep 9. Respiration. 2014. PMID: 25227115
-
Dynamics of oxygen uptake for submaximal exercise and recovery in patients with chronic heart failure.Chest. 1994 Jun;105(6):1693-700. doi: 10.1378/chest.105.6.1693. Chest. 1994. PMID: 8205862
-
Early recovery of oxygen kinetics after submaximal exercise test predicts functional capacity in patients with chronic heart failure.Eur J Heart Fail. 2001 Dec;3(6):685-92. doi: 10.1016/s1388-9842(01)00187-8. Eur J Heart Fail. 2001. PMID: 11738220
-
[The 6 minute walking test: a cost-effective alternative to spiro-ergometry in patients with chronic heart failure?].Z Kardiol. 2000 Feb;89(2):72-80. doi: 10.1007/s003920050012. Z Kardiol. 2000. PMID: 10768274 Review. German.
-
[Evaluation of exercise capacity in pulmonary arterial hypertension].Turk Kardiyol Dern Ars. 2010 Dec;38(8):580-8. Turk Kardiyol Dern Ars. 2010. PMID: 21248462 Review. Turkish.
Cited by
-
The body weight-walking distance product as a superior parameter in determining the VO2 on-kinetics in coronary artery disease.Braz J Med Biol Res. 2025 May 30;58:e14367. doi: 10.1590/1414-431X2025e14367. eCollection 2025. Braz J Med Biol Res. 2025. PMID: 40465881 Free PMC article.
-
Modeling the oxygen uptake kinetics during exercise testing of patients with chronic obstructive pulmonary diseases using nonlinear mixed models.BMC Med Res Methodol. 2016 Jun 1;16:66. doi: 10.1186/s12874-016-0173-8. BMC Med Res Methodol. 2016. PMID: 27245328 Free PMC article.
-
The reliability of VO2 kinetics during a 6-minute walking test is influenced by walk speed.J Phys Ther Sci. 2021 Dec;33(12):876-879. doi: 10.1589/jpts.33.876. Epub 2021 Dec 1. J Phys Ther Sci. 2021. PMID: 34873366 Free PMC article.
-
Underlying mechanisms of oxygen uptake kinetics in chronic post-stroke individuals: A correlational, cross-sectional pilot study.PLoS One. 2020 Nov 9;15(11):e0241872. doi: 10.1371/journal.pone.0241872. eCollection 2020. PLoS One. 2020. PMID: 33166347 Free PMC article.
-
Review of Drug Development Guidance to Treat Chronic Obstructive Pulmonary Disease: US and EU Perspectives.Clin Pharmacol Ther. 2019 Dec;106(6):1222-1235. doi: 10.1002/cpt.1540. Epub 2019 Jul 23. Clin Pharmacol Ther. 2019. PMID: 31334840 Free PMC article. Review.
References
-
- Whipp BJ, Ward SA, Lamarra N, Davis J, Wasserman K. Parameters of ventilatory and gas exchange dynamics during exercise. J Appl Physiol. 1982;52:1506. - PubMed
-
- Wasserman K, Whipp BJ, Davis JA. Respiratory Physiology of Exercise. In: Widdecombe JG, editor. International Review of Physiology, Respiratory Physiology III, vol 23. Boston: University Park Press; 1981. p. 149. - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2466/14/167/prepub
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
