

Abdominal tuberculosis of the gastrointestinal tract: revisited
- PMID: 25356043
- PMCID: PMC4209546
- DOI: 10.3748/wjg.v20.i40.14831
Abdominal tuberculosis of the gastrointestinal tract: revisited
Abstract
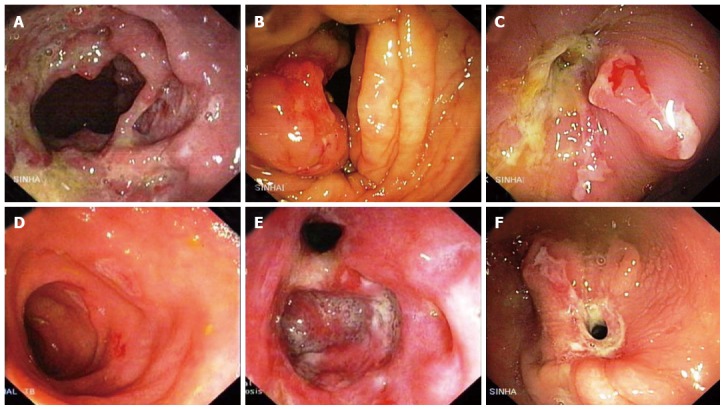
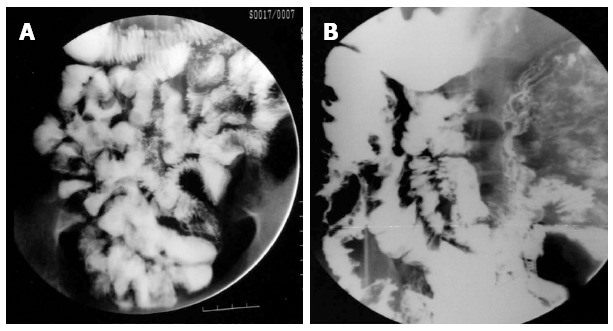
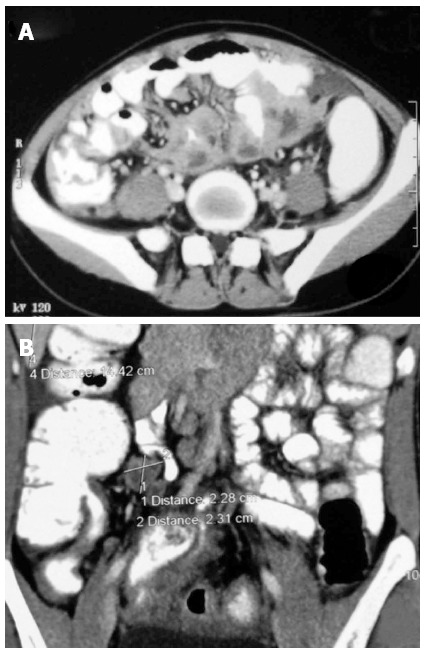
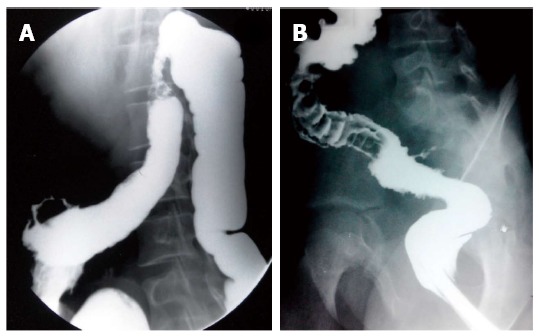
Abdominal tuberculosis is an increasingly common disease that poses diagnostic challenge, as the nonspecific features of the disease which may lead to diagnostic delays and development of complications. This condition is regarded as a great mimicker of other abdominal pathology. A high index of suspicion is an important factor in early diagnosis. Abdominal involvement may occur in the gastrointestinal tract, peritoneum, lymphnodes or solid viscera. Various investigative methods have been used to aid in the diagnosis of abdominal tuberculosis. Early diagnosis and initiation of antituberculous therapy and surgical treatment are essential to prevent morbidity and mortality. Most of the patients respond very well to standard antitubercular therapy and surgery is required only in a minority of cases. Imaging plays an important role in diagnosis of abdominal tuberculosis because early recognition of this condition is important. We reviewed our experience with the findings on various imaging modalities for diagnosis of this potentially treatable disease.
Keywords: Abdomen; Extrapulmonary; Gastrointestinal tract; Tuberculosis.
Figures




References
-
- Rosado E, Penha D, Paixao P, Costa AMD, Amadora PT. Abdominal tuberculosis - Imaging findings. Educational exhibit; ECR. 2013:C–0549.
-
- World Health Organization. Global tuberculosis report 2013. Geneva: WHO. 23 Oct; 2013. Available from: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf.
-
- Pop M, Pop C, Homorodean D, Itu C, Man M, Goron M, Gherasim R, Coroiu G. Abdominal miliary tuberculosis in a patient with AIDS: a case report. Rom J Gastroenterol. 2003;12:231–234. - PubMed
-
- Burzynski J, Schluger NW. The epidemiology of tuberculosis in the United States. Semin Respir Crit Care Med. 2008;29:492–498. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
