

Chronic Liver Failure-Sequential Organ Failure Assessment is better than the Asia-Pacific Association for the Study of Liver criteria for defining acute-on-chronic liver failure and predicting outcome
- PMID: 25356054
- PMCID: PMC4209557
- DOI: 10.3748/wjg.v20.i40.14934
Chronic Liver Failure-Sequential Organ Failure Assessment is better than the Asia-Pacific Association for the Study of Liver criteria for defining acute-on-chronic liver failure and predicting outcome
Abstract
Aim: To compare the utility of the Chronic Liver Failure-Sequential Organ Failure Assessment (CLIF-SOFA) and Asia-Pacific Association for the Study of Liver (APASL) definitions of acute-on-chronic liver failure (ACLF) in predicting short-term prognosis of patients with ACLF.
Methods: Consecutive patients of cirrhosis with acute decompensation were prospectively included. They were grouped into ACLF and no ACLF groups as per CLIF-SOFA and APASL criteria. Patients were followed up for 3 mo from inclusion or mortality whichever was earlier. Mortality at 28-d and 90-d was compared between no ACLF and ACLF groups as per both criteria. Mortality was also compared between different grades of ACLF as per CLIF-SOFA criteria. Prognostic scores like CLIF-SOFA, Acute Physiology and Chronic Health Evaluation (APACHE)-II, Child-Pugh and Model for End-Stage Liver Disease (MELD) scores were evaluated for their ability to predict 28-d mortality using area under receiver operating curves (AUROC).
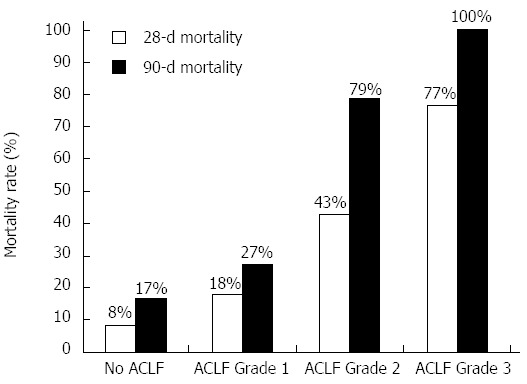
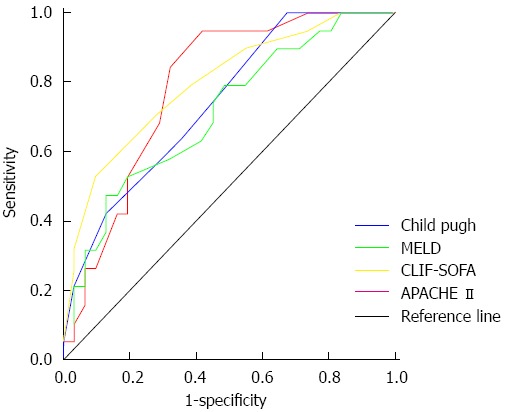
Results: Of 50 patients, 38 had ACLF as per CLIF-SOFA and 19 as per APASL criteria. Males (86%) were predominant, alcoholic liver disease (68%) was the most common etiology of cirrhosis, sepsis (66%) was the most common cause of acute decompensation while infection (66%) was the most common precipitant of acute decompensation. The 28-d mortality in no ACLF and ACLF groups was 8.3% and 47.4% (P = 0.018) as per CLIF-SOFA and 39% and 37% (P = 0.895) as per APASL criteria. The 28-d mortality in patients with no ACLF (n = 12), ACLF grade 1 (n = 11), ACLF grade 2 (n = 14) and ACLF grade 3 (n = 13) as per CLIF-SOFA criteria was 8.3%, 18.2%, 42.9% and 76.9% (χ(2) for trend, P = 0.002) and 90-d mortality was 16.7%, 27.3%, 78.6% and 100% (χ(2) for trend, P < 0.0001) respectively. Patients with prior decompensation had similar 28-d and 90-d mortality (39.3% and 53.6%) as patients without prior decompensation (36.4% and 63.6%) (P = NS). AUROCs for 28-d mortality were 0.795, 0.787, 0.739 and 0.710 for CLIF-SOFA, APACHE-II, Child-Pugh and MELD scores respectively. On multivariate analysis of these scores, CLIF-SOFA was the only significant independent predictor of mortality with an odds ratio 1.538 (95%CI: 1.078-2.194).
Conclusion: CLIF-SOFA criteria is better than APASL criteria to classify patients into ACLF based on their prognosis. CLIF-SOFA score is the best predictor of short-term mortality.
Keywords: Acute decompensation; Acute on chronic liver failure; Cirrhosis; Mortality; Prognosis.
Figures
Similar articles
-
Chronic liver failure-consortium acute-on-chronic liver failure and acute decompensation scores predict mortality in Brazilian cirrhotic patients.World J Gastroenterol. 2017 Jul 28;23(28):5237-5245. doi: 10.3748/wjg.v23.i28.5237. World J Gastroenterol. 2017. PMID: 28811718 Free PMC article.
-
Validation of prognostic scores to predict short-term mortality in patients with HBV-related acute-on-chronic liver failure: The CLIF-C OF is superior to MELD, CLIF SOFA, and CLIF-C ACLF.Medicine (Baltimore). 2017 Apr;96(17):e6802. doi: 10.1097/MD.0000000000006802. Medicine (Baltimore). 2017. PMID: 28445322 Free PMC article.
-
CLIF-SOFA scoring system accurately predicts short-term mortality in acutely decompensated patients with alcoholic cirrhosis: a retrospective analysis.Liver Int. 2015 Jan;35(1):46-57. doi: 10.1111/liv.12683. Epub 2014 Oct 1. Liver Int. 2015. PMID: 25203221 Clinical Trial.
-
Acute-on-chronic liver failure (ACLF): the 'Kyoto Consensus'-steps from Asia.Hepatol Int. 2025 Feb;19(1):1-69. doi: 10.1007/s12072-024-10773-4. Epub 2025 Feb 17. Hepatol Int. 2025. PMID: 39961976 Free PMC article. Review.
-
Prognosis algorithms for acute decompensation of cirrhosis and ACLF.Liver Int. 2025 Mar;45(3):e15927. doi: 10.1111/liv.15927. Epub 2024 Apr 9. Liver Int. 2025. PMID: 38591751 Free PMC article. Review.
Cited by
-
Current and future perspectives on acute-on-chronic liver failure: Challenges of transplantation, machine perfusion, and beyond.World J Gastroenterol. 2022 Dec 28;28(48):6922-6934. doi: 10.3748/wjg.v28.i48.6922. World J Gastroenterol. 2022. PMID: 36632319 Free PMC article. Review.
-
Impact of Hepatic and Extrahepatic Insults on the Outcome of Acute-on-Chronic Liver Failure.J Clin Exp Hepatol. 2017 Mar;7(1):9-15. doi: 10.1016/j.jceh.2016.10.006. Epub 2016 Oct 29. J Clin Exp Hepatol. 2017. PMID: 28348465 Free PMC article.
-
CLIF-SOFA and CLIF-C scores for the prognostication of acute-on-chronic liver failure and acute decompensation of cirrhosis: A systematic review.World J Hepatol. 2022 Dec 27;14(12):2025-2043. doi: 10.4254/wjh.v14.i12.2025. World J Hepatol. 2022. PMID: 36618331 Free PMC article.
-
Acute-on-chronic liver failure: Pathogenesis, prognostic factors and management.World J Gastroenterol. 2015 Nov 14;21(42):12125-40. doi: 10.3748/wjg.v21.i42.12125. World J Gastroenterol. 2015. PMID: 26576097 Free PMC article. Review.
-
Establishment of prognostic scoring models for different etiologies of acute decompensation in hospitalized patients with cirrhosis.J Int Med Res. 2019 Sep;47(9):4492-4504. doi: 10.1177/0300060519862065. Epub 2019 Jul 31. J Int Med Res. 2019. PMID: 31364441 Free PMC article.
References
-
- Olson JC, Wendon JA, Kramer DJ, Arroyo V, Jalan R, Garcia-Tsao G, Kamath PS. Intensive care of the patient with cirrhosis. Hepatology. 2011;54:1864–1872. - PubMed
-
- Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, Durand F, Gustot T, Saliba F, Domenicali M, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144:1426–137, 1426-137. - PubMed
-
- Bajaj JS. Defining acute-on-chronic liver failure: will East and West ever meet? Gastroenterology. 2013;144:1337–1339. - PubMed
-
- Moore KP, Wong F, Gines P, Bernardi M, Ochs A, Salerno F, Angeli P, Porayko M, Moreau R, Garcia-Tsao G, et al. The management of ascites in cirrhosis: report on the consensus conference of the International Ascites Club. Hepatology. 2003;38:258–266. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
