

Age-related deficit accumulation and the risk of late-life dementia
- PMID: 25356088
- PMCID: PMC4212514
- DOI: 10.1186/s13195-014-0054-5
Age-related deficit accumulation and the risk of late-life dementia
Abstract
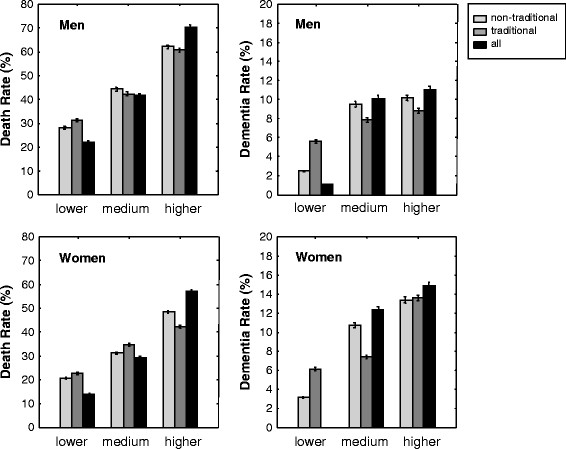
Introduction: Many age-related health problems have been associated with dementia, leading to the hypothesis that late-life dementia may be determined less by specific risk factors, and more by the operation of multiple health deficits in the aggregate. Our study addressed (a) how the predictive value of dementia risk varies by the number of deficits considered and (b) how traditional (for example. vascular risks) and nontraditional risk factors (for example, foot problems, nasal congestion) compare in their predictive effects.
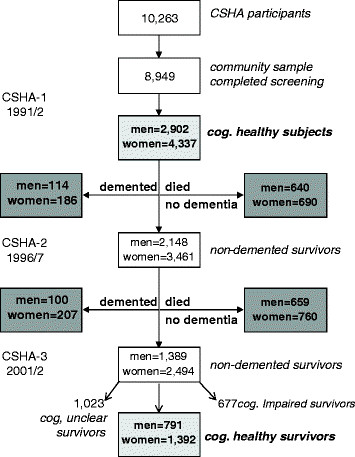
Methods: Older adults in the Canadian Study of Health and Aging who were cognitively healthy at baseline were analyzed (men, 2,902; women, 4,337). Over a 10-year period, 44.8% of men and 33.4% of women died; 7.4% of men and 9.1% of women without baseline cognitive impairment developed dementia. Self-rated health problems, including, but not restricted to, dementia risk factors, were coded as deficit present/absent. Different numbers of randomly selected variables were used to calculate various iterations of the index (that is, the proportion of deficits present in an individual. Risks for 10-year mortality and dementia outcomes were evaluated separately for men and women by using logistic regression, adjusted for age. The prediction accuracy was evaluated by using C-statistics.
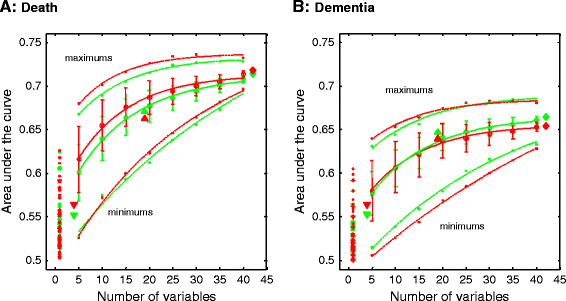
Results: Age-adjusted odds ratios per additional deficit were 1.22 (95% confidence interval (CI), 1.18 to 1.26) in men and 1.14 (1.11 to 1.16) in women in relation to death, and 1.18 (1.12 to 1.25) in men and 1.08 (1.04 to 1.11) in women in relation to dementia. The predictive value increased with the number (n) of deficits considered, regardless of whether they were known dementia risks, and stabilized at n > 25. The all-factor index best predicted dementia (C-statistics, 0.67 ± 0.03).
Conclusions: The variety of items associated with dementias suggests that some part of the risk might relate more to aberrant repair processes, than to specifically toxic results. The epidemiology of late-life illness might best consider overall health status.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
