

Meta-analysis of high- versus low-chloride content in perioperative and critical care fluid resuscitation
- PMID: 25357011
- PMCID: PMC4282059
- DOI: 10.1002/bjs.9651
Meta-analysis of high- versus low-chloride content in perioperative and critical care fluid resuscitation
Abstract
Background: The objective of this systematic review and meta-analysis was to assess the relationship between the chloride content of intravenous resuscitation fluids and patient outcomes in the perioperative or intensive care setting.
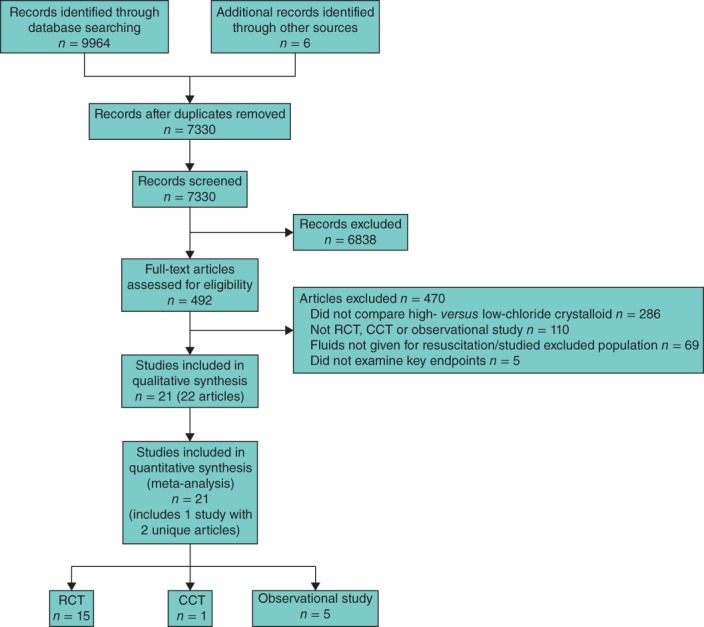
Methods: Systematic searches were performed of PubMed/MEDLINE, Embase and Cochrane Library (CENTRAL) databases in accordance with PRISMA guidelines. Randomized clinical trials, controlled clinical trials and observational studies were included if they compared outcomes in acutely ill or surgical patients receiving either high-chloride (ion concentration greater than 111 mmol/l up to and including 154 mmol/l) or lower-chloride (concentration 111 mmol/l or less) crystalloids for resuscitation. Endpoints examined were mortality, measures of kidney function, serum chloride, hyperchloraemia/metabolic acidosis, blood transfusion volume, mechanical ventilation time, and length of hospital and intensive care unit stay. Risk ratios (RRs), mean differences (MDs) or standardized mean differences (SMDs) and confidence intervals were calculated using fixed-effect modelling.
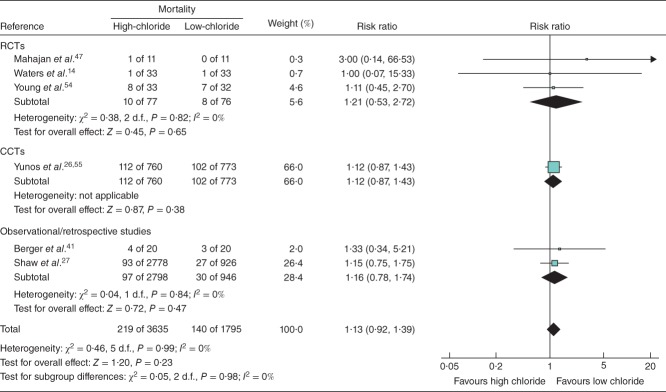
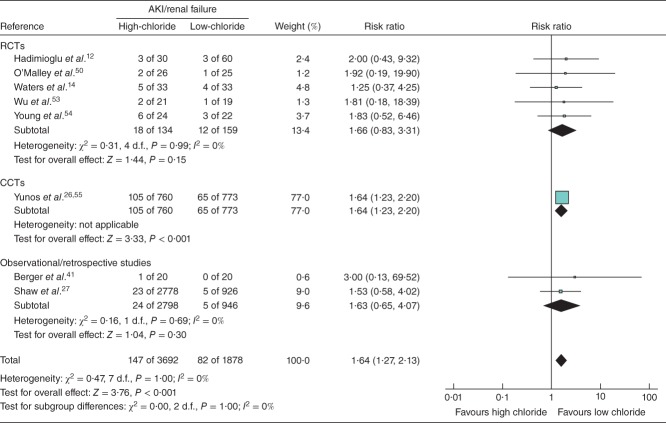
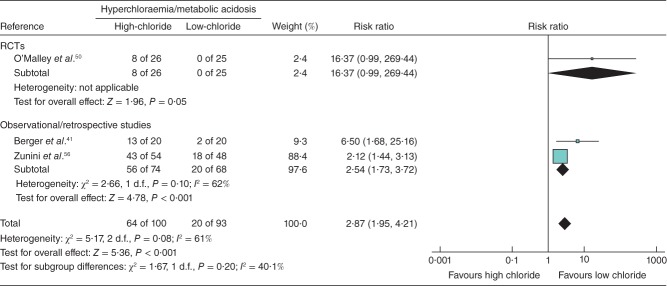
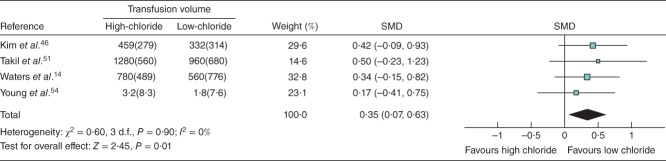
Results: The search identified 21 studies involving 6253 patients. High-chloride fluids did not affect mortality but were associated with a significantly higher risk of acute kidney injury (RR 1.64, 95 per cent c.i. 1.27 to 2.13; P < 0.001) and hyperchloraemia/metabolic acidosis (RR 2.87, 1.95 to 4.21; P < 0.001). High-chloride fluids were also associated with greater serum chloride (MD 3.70 (95 per cent c.i. 3.36 to 4.04) mmol/l; P < 0.001), blood transfusion volume (SMD 0.35, 0.07 to 0.63; P = 0.014) and mechanical ventilation time (SMD 0.15, 0.08 to 0.23; P < 0.001). Sensitivity analyses excluding heavily weighted studies resulted in non-statistically significant effects for acute kidney injury and mechanical ventilation time.
Conclusion: A weak but significant association between higher chloride content fluids and unfavourable outcomes was found, but mortality was unaffected by chloride content.
© 2014 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Comment in
-
The hidden costs of normal saline: Increased transfusions and vasopressor infusions.J Clin Anesth. 2023 Sep;88:111141. doi: 10.1016/j.jclinane.2023.111141. Epub 2023 May 9. J Clin Anesth. 2023. PMID: 37167797 No abstract available.
References
-
- Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013;369:1243–1251. - PubMed
-
- Veech RL. The toxic impact of parenteral solutions on the metabolism of cells: a hypothesis for physiological parenteral therapy. Am J Clin Nutr. 1986;44:519–551. - PubMed
-
- Ho AM, Karmakar MK, Contardi LH, Ng SS, Hewson JR. Excessive use of normal saline in managing traumatized patients in shock: a preventable contributor to acidosis. J Trauma. 2001;51:173–177. - PubMed
-
- Awad S, Allison SP, Lobo DN. The history of 0·9% saline. Clin Nutr. 2008;27:179–188. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
