

Efficacy and safety of pateclizumab (anti-lymphotoxin-α) compared to adalimumab in rheumatoid arthritis: a head-to-head phase 2 randomized controlled study (The ALTARA Study)
- PMID: 25359150
- PMCID: PMC4243296
- DOI: 10.1186/s13075-014-0467-3
Efficacy and safety of pateclizumab (anti-lymphotoxin-α) compared to adalimumab in rheumatoid arthritis: a head-to-head phase 2 randomized controlled study (The ALTARA Study)
Abstract
Introduction: Tumor necrosis factor (TNF) and, possibly, lymphotoxin alpha (LTα) signaling contribute to inflammation and rheumatoid arthritis (RA) pathogenesis. Pateclizumab (anti-lymphotoxin- alpha; MLTA3698A) is a humanized monoclonal antibody that blocks and depletes anti-LTα. This phase 2, randomized, head-to-head, active- and placebo-controlled trial examined the safety and efficacy of pateclizumab compared to adalimumab in RA patients with an inadequate response to disease-modifying antirheumatic drugs (DMARD-IR).
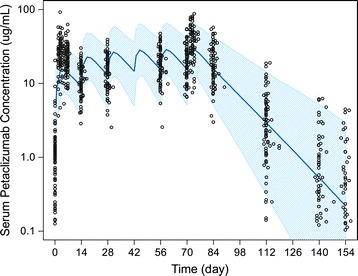
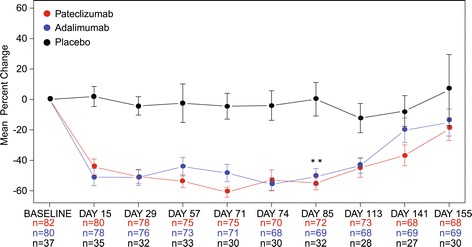
Methods: Patients (n = 214) with active RA (≥ 6 swollen and tender joints, C-reactive protein ≥ 10 mg/L) on oral DMARDs were randomized (2:2:1) to receive pateclizumab 360 mg, adalimumab 40 mg, or placebo subcutaneously every 2 weeks. The primary endpoint, 4-variable, 28-joint disease activity score erythrocyte sedimentation rate (DAS28(4)-ESR) response, was evaluated at 12 weeks using an analysis of covariance (ANCOVA) model with adjustments for concomitant DMARD use and geographic region. Secondary efficacy endpoints included American College of Rheumatology (ACR) 20, ACR50, and ACR70 responses at Day 85. Pharmacokinetics, pharmacodynamics, and immunogenicity of pateclizumab were assessed.
Results: Pateclizumab reduced the DAS28(4)-ESR response (-1.89) at 12 weeks, however, this did not reach statistical significance compared to placebo (-1.54), while adalimumab (-2.52) differed significantly from both placebo and pateclizumab. Pateclizumab 12-week ACR20, ACR50 and ACR70 response rates (64%, 33%, and 14%) suggested clinical activity but were not statistically significant compared to placebo rates (46%, 24%, and 8%, respectively). CXCL13 serum levels decreased significantly following pateclizumab and adalimumab administration, demonstrating pharmacological target engagement by both drugs. Overall, adverse events (AEs) were comparable among all cohorts. Infections were the most common AE, occurring with comparable frequency in all groups. Serious AEs occurred in 0% of pateclizumab, 5.9% of adalimumab, and 2.3% of placebo patients, with serious infection in 2.3% of adalimumab patients and none in pateclizumab and placebo patients.
Conclusions: Pateclizumab had a good safety profile in patients inadequately responsive to DMARDs, but no statistically significant improvement in RA signs and symptoms after 12 weeks of treatment. Adalimumab demonstrated efficacy and safety comparable to published results in this head-to-head comparison in DMARD-IR RA patients.
Trial registration: ClinicalTrials.gov NCT01225393, Registered 18 October 2010.
Figures
References
-
- Smolen JS, Landewé R, Breedveld FC, Buch M, Burmester G, Dougados M, Emery P, Gaujoux-Viala C, Gossec L, Nam J, Ramiro S, Winthrop K, de Wit M, Aletaha D, Betteridge N, Bijlsma JW, Boers M, Buttgereit F, Combe B, Cutolo M, Damjanov N, Hazes JM, Kouloumas M, Kvien TK, Mariette X, Pavelka, van Riel PL, Rubbert-Roth A, Scholte-Voshaar M, Scott DL, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis. 2014;73:492–509. doi: 10.1136/annrheumdis-2013-204573. - DOI - PMC - PubMed
-
- Chiang EY, Kolumam GA, Yu X, Francesco M, Ivelja S, Peng I, Gribling P, Shu J, Lee WP, Refino CJ, Balazs M, Paler-Martinez A, Nguyen A, Young J, Barck KH, Carano RA, Ferrando R, Diehl L, Chatterjea D, Grogan JL. Targeted depletion of lymphotoxin-alpha-expressing TH1 and TH17 cells inhibits autoimmune disease. Nat Med. 2009;15:766–773. doi: 10.1038/nm.1984. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
