

Multidetector computed tomography of mesenteric ischaemia
- PMID: 25359530
- PMCID: PMC4263800
- DOI: 10.1007/s13244-014-0361-1
Multidetector computed tomography of mesenteric ischaemia
Abstract
Mesenteric ischaemia comprises a broad, heterogeneous group of diseases characterised by inadequate blood supply to the small or large bowel. Acute mesenteric ischaemia is a surgical emergency, with significant associated morbidity and mortality. Because the clinical presentation of mesenteric ischaemia is variable and often nonspecific, a high index of clinical and radiologic suspicion is required for early diagnosis. The severity of mesenteric ischaemia ranges from transient, localised ischaemia to frank necrosis of the bowel. The most common causes of acute mesenteric ischaemia are embolic and thrombotic occlusion of the superior mesenteric artery, whereas chronic mesenteric ischaemia is almost always associated with generalised atherosclerotic disease. Multidetector computed tomography (MDCT) angiography is the preferred imaging test for acute and chronic mesenteric ischaemia. MDCT is useful in making a prompt, more precise diagnosis of mesenteric ischaemia, as well as identifying the cause and potential complications, which are key to reducing patient morbidity and mortality. In this article, we review the clinical features and aetiologies of mesenteric ischaemia and illustrate the imaging manifestations on MDCT.
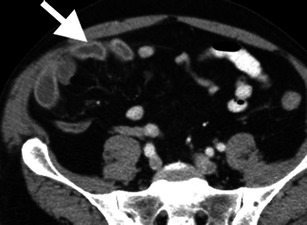
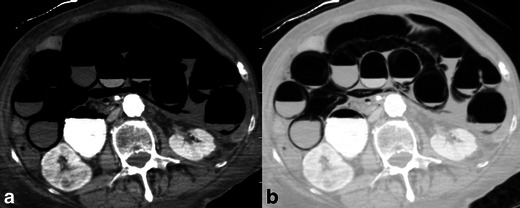
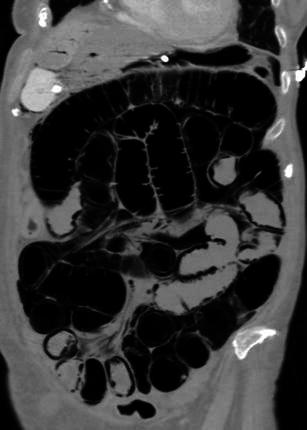
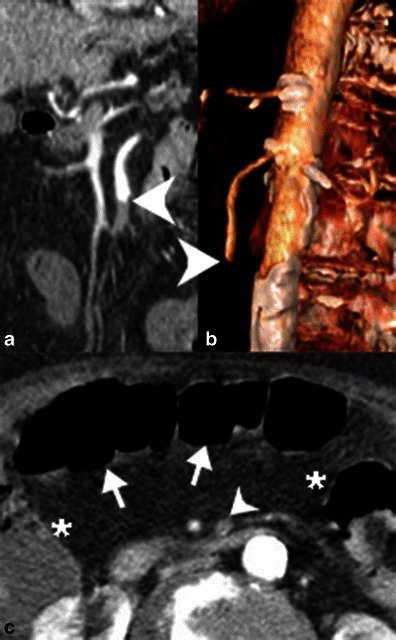
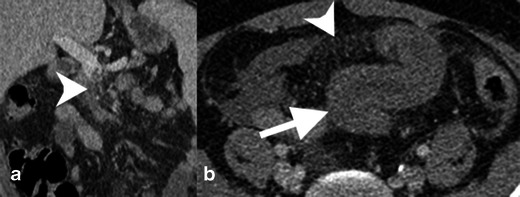
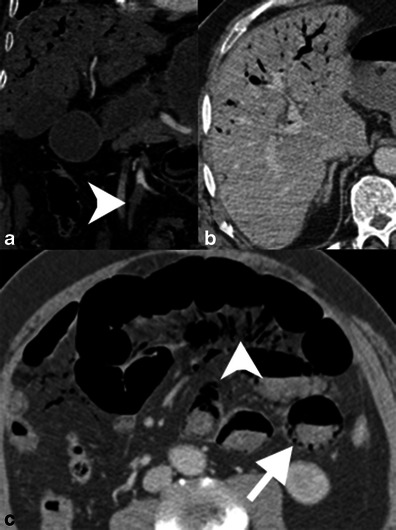
Main messages: • Acute and chronic mesenteric ischaemia are morbid conditions challenging to diagnose. • MDCT is the first-line imaging test for evaluating patients with suspected mesenteric ischaemia. • Bowel findings include wall thickening, abnormal enhancement, pneumatosis and luminal dilation. • Vascular occlusion, portomesenteric venous gas, mesenteric congestion and free air can be seen.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
