

Clinical challenges of chronic wounds: searching for an optimal animal model to recapitulate their complexity
- PMID: 25359790
- PMCID: PMC4213725
- DOI: 10.1242/dmm.016782
Clinical challenges of chronic wounds: searching for an optimal animal model to recapitulate their complexity
Abstract
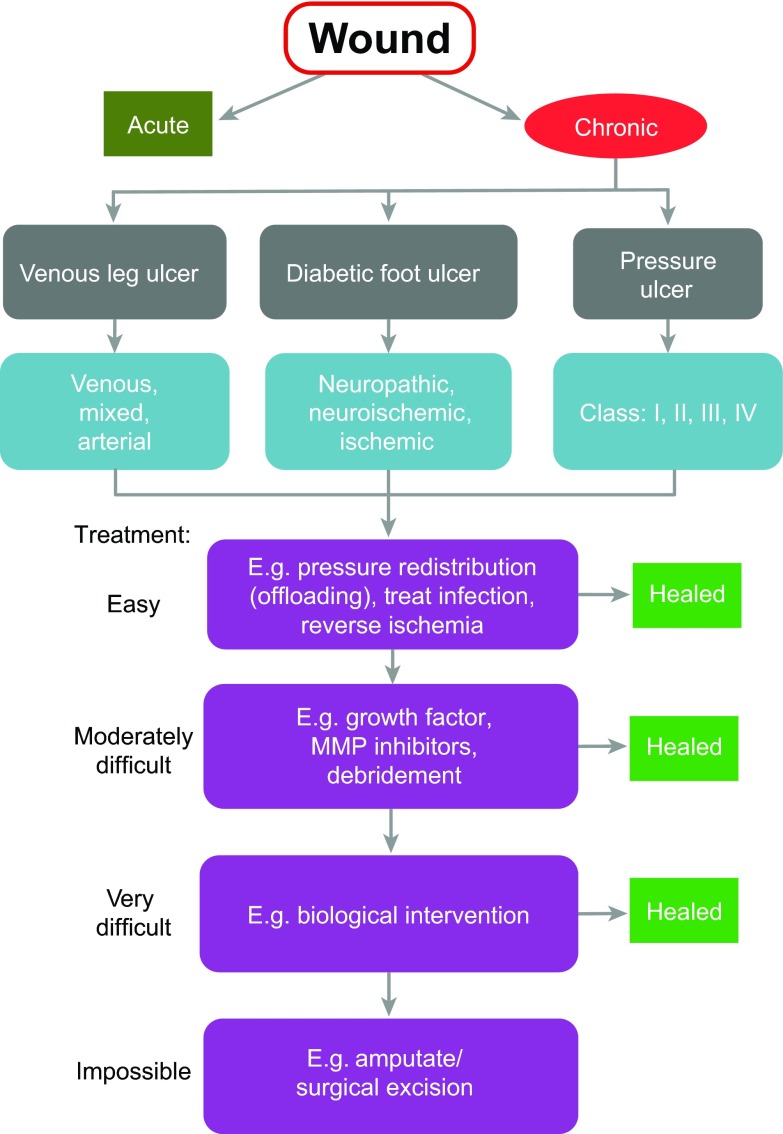
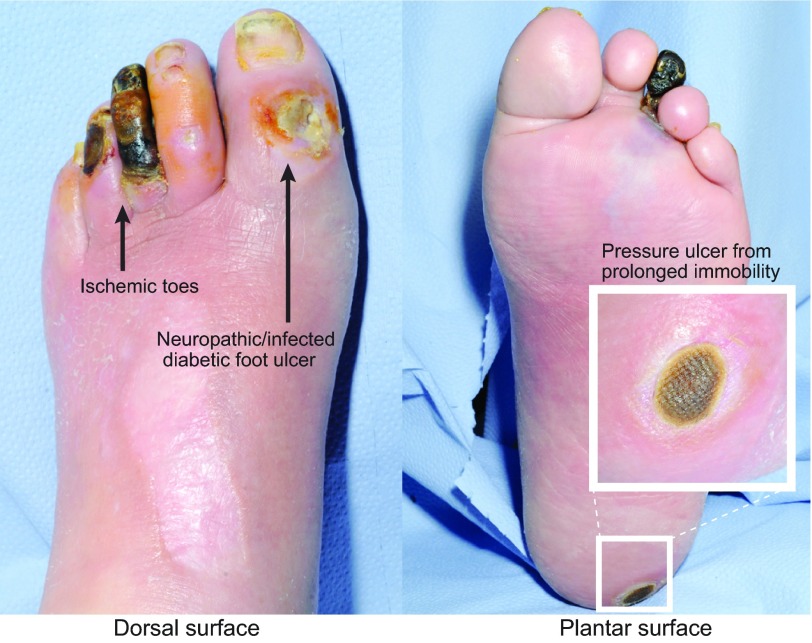
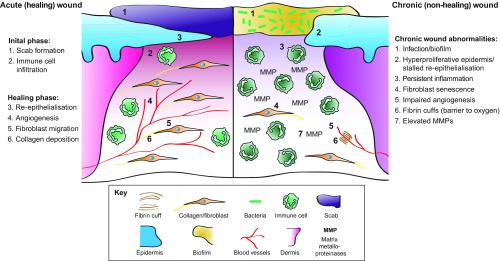
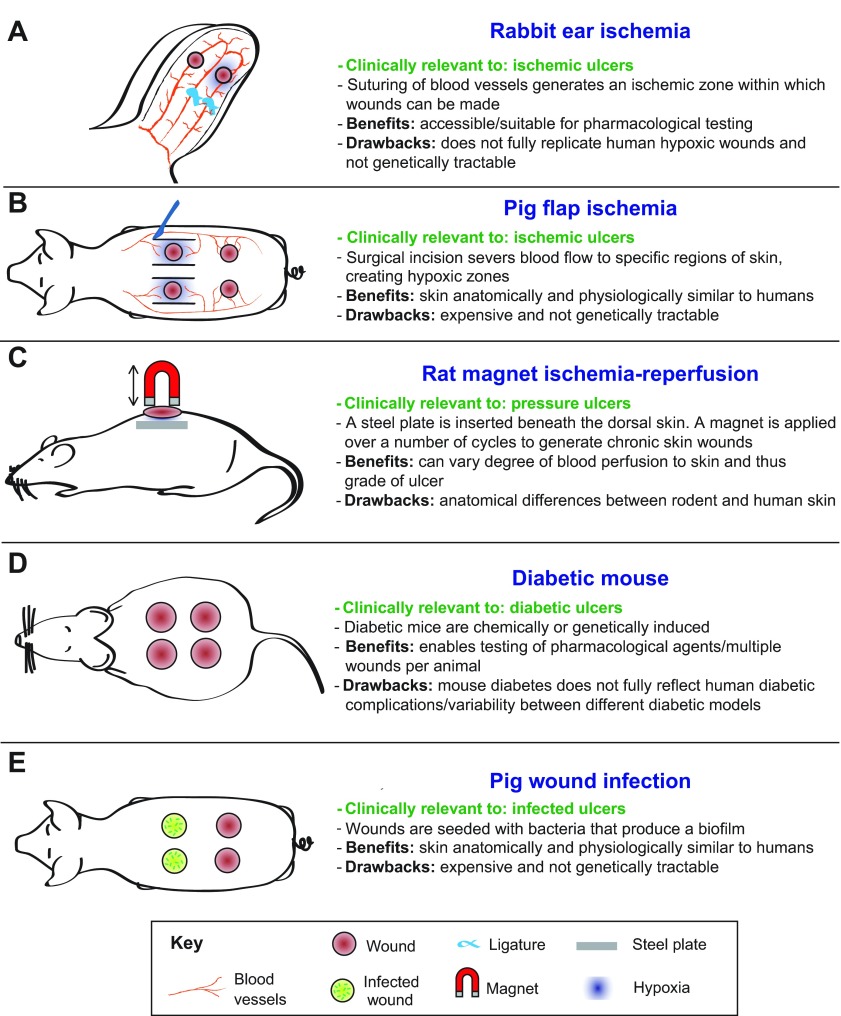
The efficient healing of a skin wound is something that most of us take for granted but is essential for surviving day-to-day knocks and cuts, and is absolutely relied on clinically whenever a patient receives surgical intervention. However, the management of a chronic wound - defined as a barrier defect that has not healed in 3 months - has become a major therapeutic challenge throughout the Western world, and it is a problem that will only escalate with the increasing incidence of conditions that impede wound healing, such as diabetes, obesity and vascular disorders. Despite being clinically and molecularly heterogeneous, all chronic wounds are generally assigned to one of three major clinical categories: leg ulcers, diabetic foot ulcers or pressure ulcers. Although we have gleaned much knowledge about the fundamental cellular and molecular mechanisms that underpin healthy, acute wound healing from various animal models, we have learned much less about chronic wound repair pathology from these models. This might largely be because the animal models being used in this field of research have failed to recapitulate the clinical features of chronic wounds. In this Clinical Puzzle article, we discuss the clinical complexity of chronic wounds and describe the best currently available models for investigating chronic wound pathology. We also assess how such models could be optimised to become more useful tools for uncovering pathological mechanisms and potential therapeutic treatments.
Keywords: Animal models; Chronic wounds; Diabetic foot ulcer; Ischemia; Pressure ulcer; Venous leg ulcer.
© 2014. Published by The Company of Biologists Ltd.
Figures
References
-
- Ahn S. T., Mustoe T. A. (1990). Effects of ischemia on ulcer wound healing: a new model in the rabbit ear. Ann. Plast. Surg. 24, 17–23 - PubMed
-
- Apelqvist J., Larsson J., Agardh C. D. (1993). Long-term prognosis for diabetic patients with foot ulcers. J. Intern. Med. 233, 485–491 - PubMed
-
- Barwell J. R., Davies C. E., Deacon J., Harvey K., Minor J., Sassano A., Taylor M., Usher J., Wakely C., Earnshaw J. J., et al. (2004). Comparison of surgery and compression with compression alone in chronic venous ulceration (ESCHAR study): randomised controlled trial. Lancet 363, 1854–1859 - PubMed
-
- Bennett G., Dealey C., Posnett J. (2004). The cost of pressure ulcers in the UK. Age Ageing 33, 230–235 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
