

β-Blocker dialyzability and mortality in older patients receiving hemodialysis
- PMID: 25359874
- PMCID: PMC4378109
- DOI: 10.1681/ASN.2014040324
β-Blocker dialyzability and mortality in older patients receiving hemodialysis
Abstract
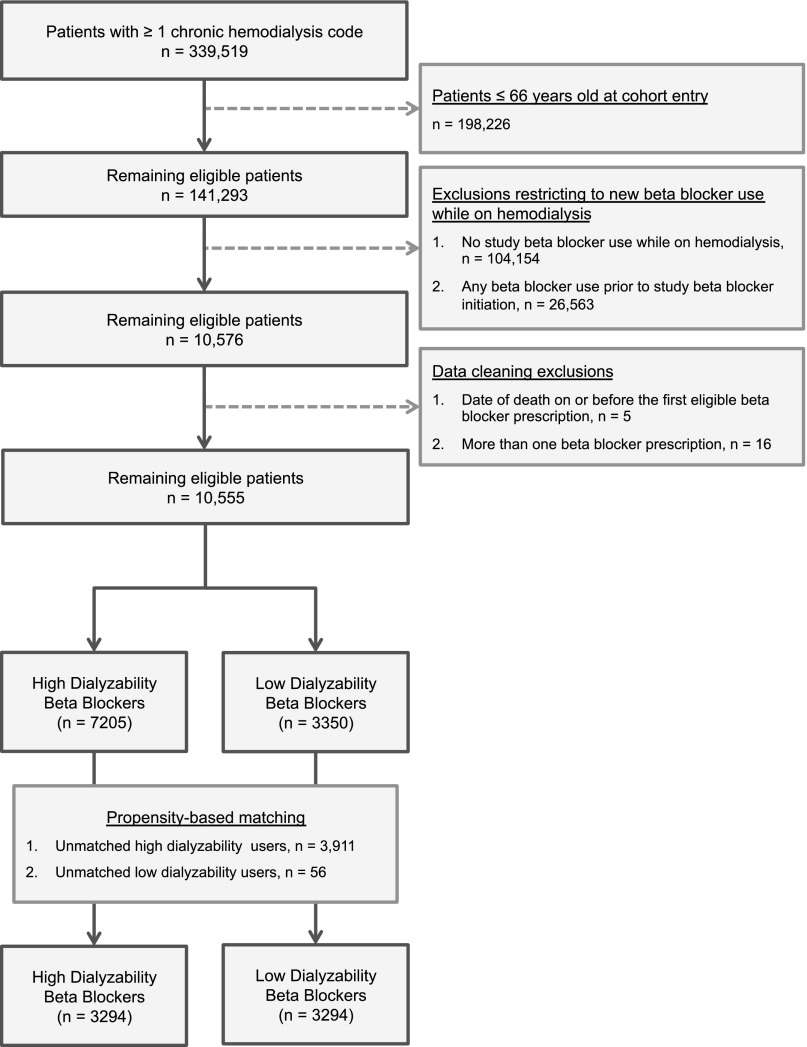
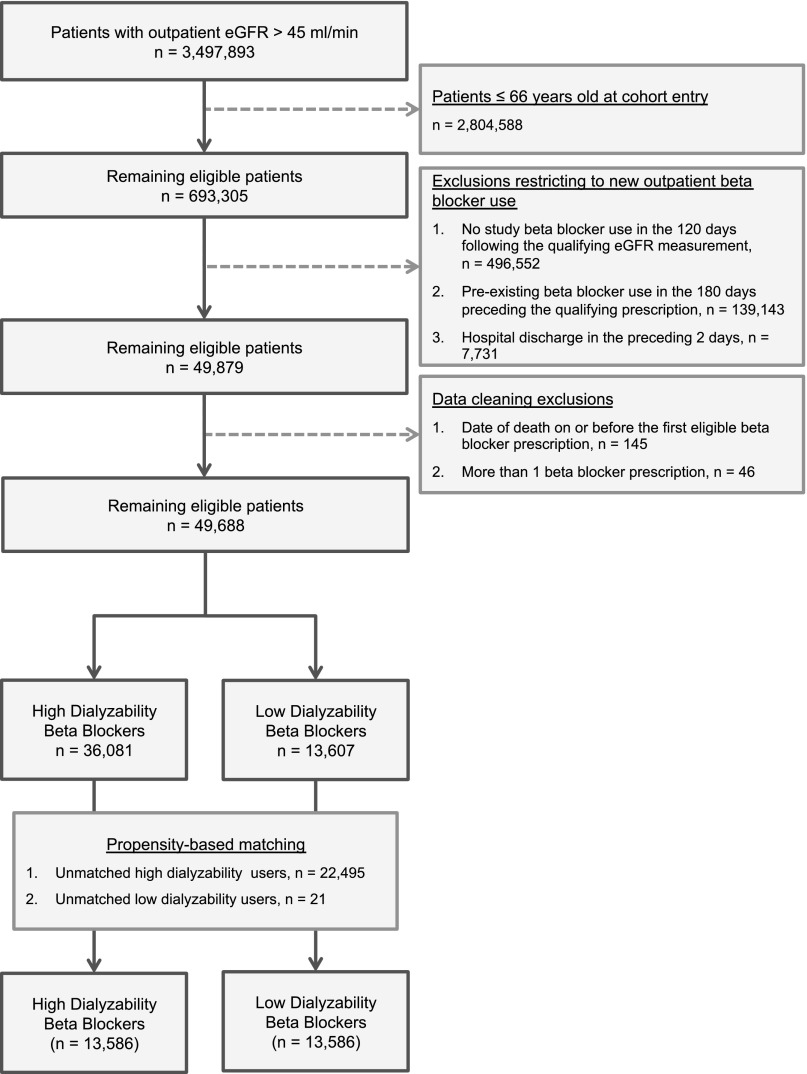
Some β-blockers are efficiently removed from the circulation by hemodialysis ("high dialyzability") whereas others are not ("low dialyzability"). This characteristic may influence the effectiveness of the β-blockers among patients receiving long-term hemodialysis. To determine whether new use of a high-dialyzability β-blocker compared with a low-dialyzability β-blocker associates with a higher rate of mortality in patients older than age 66 years receiving long-term hemodialysis, we conducted a propensity-matched population-based retrospective cohort study using the linked healthcare databases of Ontario, Canada. The high-dialyzability group (n=3294) included patients initiating atenolol, acebutolol, or metoprolol. The low-dialyzability group (n=3294) included patients initiating bisoprolol or propranolol. Initiation of a high- versus low-dialyzability β-blocker was associated with a higher risk of death in the following 180 days (relative risk, 1.4; 95% confidence interval, 1.1 to 1.8; P<0.01). Supporting this finding, we repeated the primary analysis in a cohort of patients not receiving hemodialysis and found no significant association between dialyzability and the risk of death (relative risk, 1.0; 95% confidence interval, 0.9 to 1.3; P=0.71). β-Blocker exposure was not randomly allocated in this study, so a causal relationship between dialyzability and mortality cannot be determined. However, our findings should raise awareness of this potentially important drug characteristic and prompt further study.
Keywords: cardiovascular disease; hemodialysis; mortality; pharmacokinetics.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
- 774–776 doi: 10.1681/ASN.2014080831
References
-
- Wanner C, Krane V, März W, Olschewski M, Mann JFE, Ruf G, Ritz E, German Diabetes and Dialysis Study Investigators : Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N Engl J Med 353: 238–248, 2005 - PubMed
-
- K/DOQI Workgroup : K/DOQI clinical practice guidelines for cardiovascular disease in dialysis patients. Am J Kidney Dis 45: S1–153, 2005 - PubMed
-
- Roux A, Aubert P, Guedon J, Flouvat B: Pharmacokinetics of acebutolol in patients with all grades of renal failure. Eur J Clin Pharmacol 17: 339–348, 1980 - PubMed
-
- Campese VM, Feinstein EI, Gura V, Mason WD, Massry SG: Pharmacokinetics of atenolol in patients treated with chronic hemodialysis or peritoneal dialysis. J Clin Pharmacol 25: 393–395, 1985 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
