

Team Learning for Healthcare Quality Improvement
- PMID: 25360395
- PMCID: PMC4211024
- DOI: 10.1109/ACCESS.2013.2280086
Team Learning for Healthcare Quality Improvement
Abstract
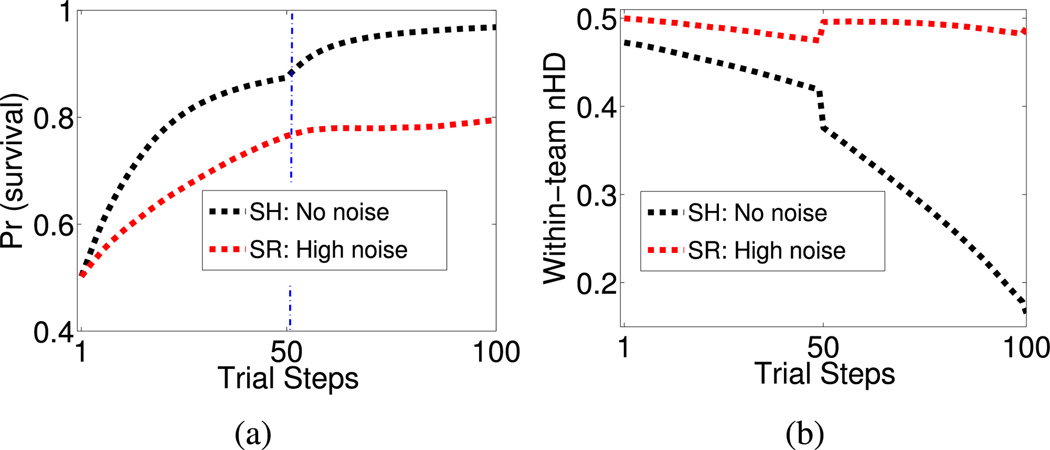
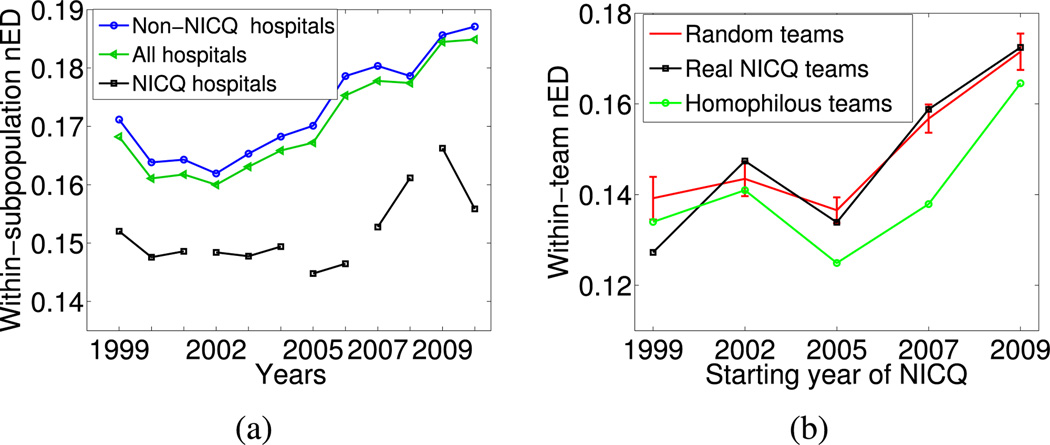
In organized healthcare quality improvement collaboratives (QICs), teams of practitioners from different hospitals exchange information on clinical practices with the aim of improving health outcomes at their own institutions. However, what works in one hospital may not work in others with different local contexts because of nonlinear interactions among various demographics, treatments, and practices. In previous studies of collaborations where the goal is a collective problem solving, teams of diverse individuals have been shown to outperform teams of similar individuals. However, when the purpose of collaboration is knowledge diffusion in complex environments, it is not clear whether team diversity will help or hinder effective learning. In this paper, we first use an agent-based model of QICs to show that teams comprising similar individuals outperform those with more diverse individuals under nearly all conditions, and that this advantage increases with the complexity of the landscape and level of noise in assessing performance. Examination of data from a network of real hospitals provides encouraging evidence of a high degree of similarity in clinical practices, especially within teams of hospitals engaging in QIC teams. However, our model also suggests that groups of similar hospitals could benefit from larger teams and more open sharing of details on clinical outcomes than is currently the norm. To facilitate this, we propose a secure virtual collaboration system that would allow hospitals to efficiently identify potentially better practices in use at other institutions similar to theirs without any institutions having to sacrifice the privacy of their own data. Our results may also have implications for other types of data-driven diffusive learning such as in personalized medicine and evolutionary search in noisy, complex combinatorial optimization problems.
Keywords: Agent-based modeling; collaborative learning; healthcare quality; knowledge diffusion; quality improvement; team collaboration; team learning.
Figures










References
-
- Cohen P, Levesque H. “Teamwork,”. Nous. 1991;1991;25(4):487–512.
-
- West M. Effective Teamwork: Practical Lessons from Organizational Research. Oxford, U.K.: Blackwell; 2012.
-
- Poulton B, West M. “Effective multidisciplinary teamwork in primary health care,”. J. Adv. Nursing. 2008;18(6):918–925. - PubMed
-
- Turner M. Groups at Work: Theory and Research. Hillsdale, NJ, USA: Lawrence Erlbaum; 2000.
-
- LePine J, Piccolo R, Jackson C, Mathieu J, Saul J. “A metaanalysis of teamwork processes: Tests of a multidimensional model and relationships with team effectiveness criteria,”. Personnel Psychol. 2008;2008;61(2):213–301.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources