

Elevated levels of monocyte activation markers are associated with subclinical atherosclerosis in men with and those without HIV infection
- PMID: 25362192
- PMCID: PMC4402336
- DOI: 10.1093/infdis/jiu594
Elevated levels of monocyte activation markers are associated with subclinical atherosclerosis in men with and those without HIV infection
Abstract
Background: Heightened immune activation among human immunodeficiency virus (HIV)-infected persons may contribute to atherosclerosis. We assessed associations of serologic markers of monocyte activation, soluble CD163 (sCD163) and soluble CD14 (sCD14), and monocyte chemoattractant protein 1 (CCL2) with subclinical atherosclerosis among men with and those without HIV infection in the Multicenter AIDS Cohort Study.
Methods: We performed noncontrast computed tomography on 906 men (566 HIV-infected men and 340 HIV-uninfected men), 709 of whom also underwent coronary computed tomographic angiography. Associations between each biomarker and the prevalence of coronary plaque, the prevalence of stenosis of ≥50%, and the extent of plaque were assessed by logistic and linear regression, adjusting for age, race, HIV serostatus, and cardiovascular risk factors.
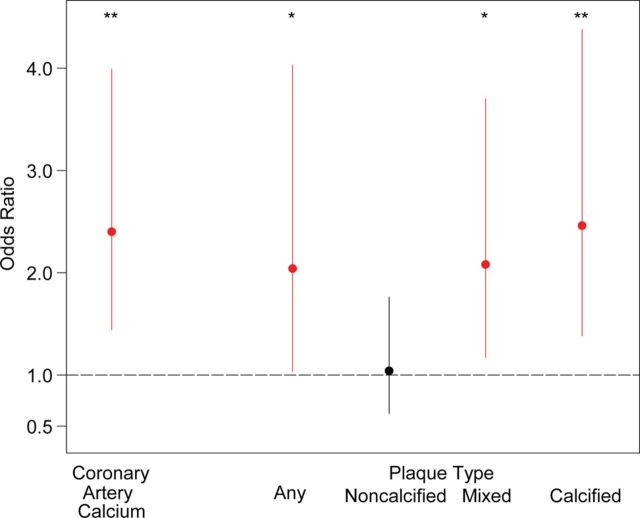
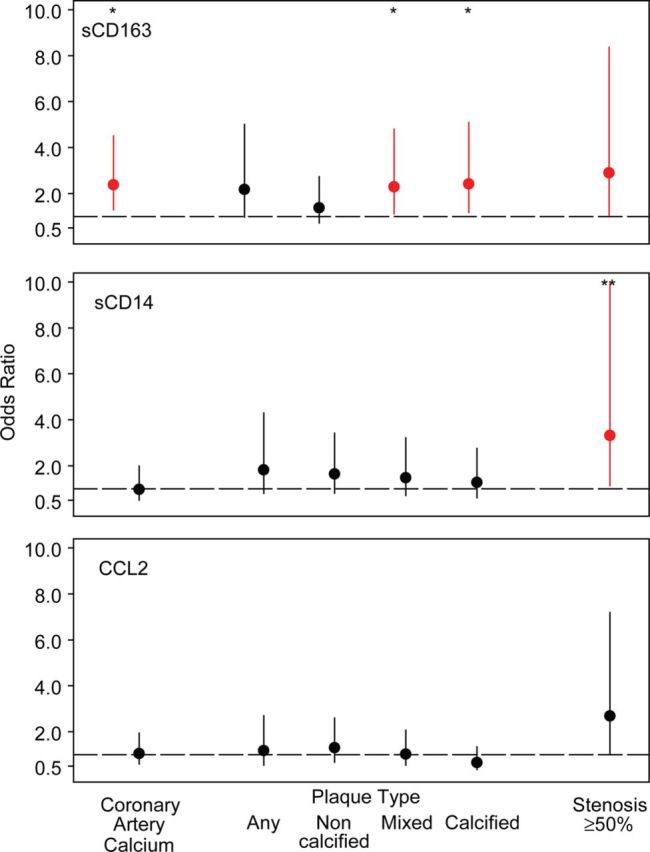
Results: Levels of all biomarkers were higher among HIV-infected men, of whom 81% had undetectable HIV RNA, and were associated with lower CD4(+) T-cell counts. In the entire population and among HIV-infected men, higher biomarker levels were associated with a greater prevalence of coronary artery stenosis of ≥50%. Higher sCD163 levels were also associated with greater prevalences of coronary artery calcium, mixed plaque, and calcified plaque; higher CCL2 levels were associated with a greater extent of noncalcified plaque.
Conclusions: sCD163, sCD14, and CCL2 levels were elevated in treated HIV-infected men and associated with atherosclerosis. Monocyte activation may increase the risk for cardiovascular disease in individuals with HIV infection.
Keywords: atherosclerosis; human immunodeficiency virus; inflammation; monocyte activation; plaque.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures

Similar articles
-
Soluble CD163, a novel marker of activated macrophages, is elevated and associated with noncalcified coronary plaque in HIV-infected patients.J Infect Dis. 2011 Oct 15;204(8):1227-36. doi: 10.1093/infdis/jir520. J Infect Dis. 2011. PMID: 21917896 Free PMC article.
-
Noncalcified coronary atherosclerotic plaque and immune activation in HIV-infected women.J Infect Dis. 2013 Dec 1;208(11):1737-46. doi: 10.1093/infdis/jit508. Epub 2013 Sep 16. J Infect Dis. 2013. PMID: 24041790 Free PMC article.
-
Subclinical cardiovascular disease in HIV controller and long-term nonprogressor populations.HIV Med. 2020 Apr;21(4):217-227. doi: 10.1111/hiv.12820. Epub 2019 Nov 14. HIV Med. 2020. PMID: 31729142 Free PMC article.
-
B cells and atherosclerosis: A HIV perspective.J Cell Physiol. 2024 Jun;239(6):e31270. doi: 10.1002/jcp.31270. Epub 2024 Apr 23. J Cell Physiol. 2024. PMID: 38651687 Free PMC article. Review.
-
Coronary Artery Disease Manifestations in HIV: What, How, and Why.Can J Cardiol. 2019 Mar;35(3):270-279. doi: 10.1016/j.cjca.2018.11.029. Epub 2018 Dec 4. Can J Cardiol. 2019. PMID: 30825949 Free PMC article. Review.
Cited by
-
HIV-1 Persistence and Chronic Induction of Innate Immune Responses in Macrophages.Viruses. 2020 Jun 30;12(7):711. doi: 10.3390/v12070711. Viruses. 2020. PMID: 32630058 Free PMC article. Review.
-
HIV Infection and Carotid Artery Intima-media Thickness: Pooled Analyses Across 5 Cohorts of the NHLBI HIV-CVD Collaborative.Clin Infect Dis. 2016 Jul 15;63(2):249-56. doi: 10.1093/cid/ciw261. Epub 2016 Apr 26. Clin Infect Dis. 2016. PMID: 27118787 Free PMC article.
-
Elevated Autotaxin and LPA Levels During Chronic Viral Hepatitis and Hepatocellular Carcinoma Associate with Systemic Immune Activation.Cancers (Basel). 2019 Nov 25;11(12):1867. doi: 10.3390/cancers11121867. Cancers (Basel). 2019. PMID: 31769428 Free PMC article. Review.
-
Targeting Inflammation to Reduce Atherosclerotic Cardiovascular Risk in People With HIV Infection.J Am Heart Assoc. 2020 Feb 4;9(3):e014873. doi: 10.1161/JAHA.119.014873. Epub 2020 Jan 24. J Am Heart Assoc. 2020. PMID: 31973607 Free PMC article. Review. No abstract available.
-
Ageing with HIV.Healthcare (Basel). 2018 Feb 14;6(1):17. doi: 10.3390/healthcare6010017. Healthcare (Basel). 2018. PMID: 29443936 Free PMC article. Review.
References
-
- May MT, Sterne JA, Costagliola D, et al. HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis. Lancet 2006; 368:451–8. - PubMed
-
- Palella FJ, Jr., Baker RK, Moorman AC, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr 2006; 43:27–34. - PubMed
-
- Currier JS, Taylor A, Boyd F, et al. Coronary heart disease in HIV-infected individuals. J Acquir Immune Defic Syndr 2003; 33:506–12. - PubMed
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Munoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984–2008. Am J Epidemiol 2013; 177:116–25. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 AI035042/AI/NIAID NIH HHS/United States
- P30 DK040561/DK/NIDDK NIH HHS/United States
- UL1-TR000124/TR/NCATS NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- UO1-AI-35042/AI/NIAID NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- 5R01 HL095126/HL/NHLBI NIH HHS/United States
- R01 HL095129/HL/NHLBI NIH HHS/United States
- UL1-RR025005/RR/NCRR NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- UO1-AI-35040/AI/NIAID NIH HHS/United States
- K24 AI120834/AI/NIAID NIH HHS/United States
- R01 HL095126/HL/NHLBI NIH HHS/United States
- UO1-AI-35041/AI/NIAID NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- UM1-AI-35043/AI/NIAID NIH HHS/United States
- UO1-AI-35039/AI/NIAID NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
