

Neurocognitive change in the era of HIV combination antiretroviral therapy: the longitudinal CHARTER study
- PMID: 25362201
- PMCID: PMC4303775
- DOI: 10.1093/cid/ciu862
Neurocognitive change in the era of HIV combination antiretroviral therapy: the longitudinal CHARTER study
Abstract
Background: Human immunodeficiency virus (HIV)-associated neurocognitive disorders (HAND) can show variable clinical trajectories. Previous longitudinal studies of HAND typically have been brief, did not use adequate normative standards, or were conducted in the context of a clinical trial, thereby limiting our understanding of incident neurocognitive (NC) decline and recovery.
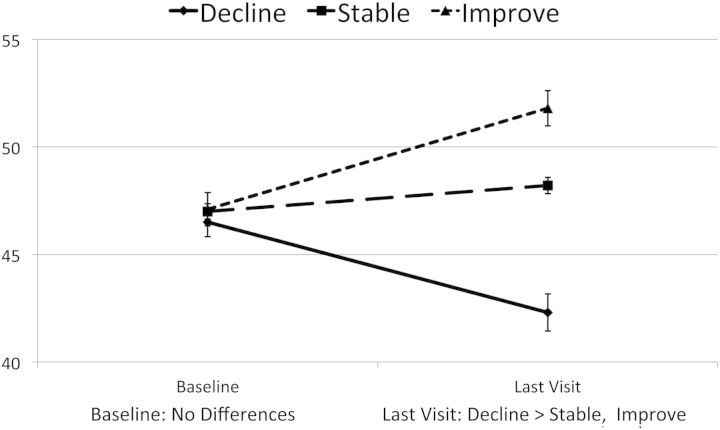
Methods: We investigated the incidence and predictors of NC change over 16-72 (mean, 35) months in 436 HIV-infected participants in the CNS HIV Anti-Retroviral Therapy Effects Research cohort. Comprehensive laboratory, neuromedical, and NC assessments were obtained every 6 months. Published, regression-based norms for NC change were used to generate overall change status (decline vs stable vs improved) at each study visit. Survival analysis was used to examine the predictors of time to NC change.
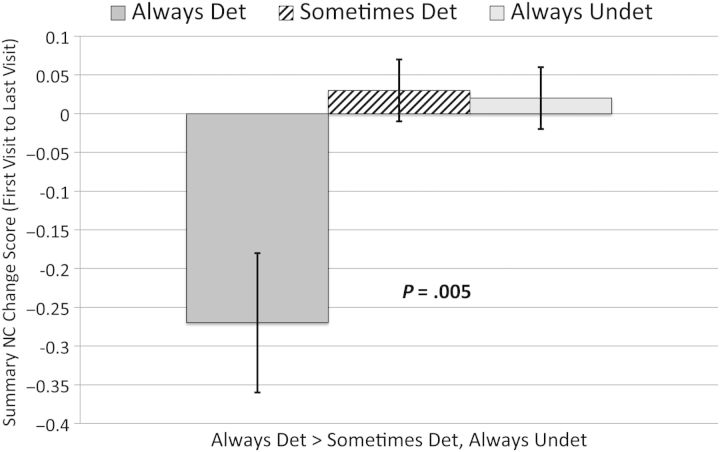
Results: Ninety-nine participants (22.7%) declined, 265 (60.8%) remained stable, and 72 (16.5%) improved. In multivariable analyses, predictors of NC improvements or declines included time-dependent treatment status and indicators of disease severity (current hematocrit, albumin, total protein, aspartate aminotransferase), and baseline demographics and estimated premorbid intelligence quotient, non-HIV-related comorbidities, current depressive symptoms, and lifetime psychiatric diagnoses (overall model P < .0001).
Conclusions: NC change is common in HIV infection and appears to be driven by a complex set of risk factors involving HIV disease, its treatment, and comorbid conditions.
Keywords: HIV; antiretroviral therapy; cognitive change; comorbidities.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Should longitudinal multisite studies become the new standard for investigating neurocognitive functions in HIV infection?Clin Infect Dis. 2015 Feb 1;60(3):481-2. doi: 10.1093/cid/ciu863. Epub 2014 Oct 31. Clin Infect Dis. 2015. PMID: 25362203 No abstract available.
-
Neurocognitive change observed in the CHARTER HIV cohort could be due to chance, and may be a cause as well as a consequence of detectable viremia.Clin Infect Dis. 2015 May 1;60(9):1441-2. doi: 10.1093/cid/civ043. Epub 2015 Feb 2. Clin Infect Dis. 2015. PMID: 25645215 No abstract available.
-
Reply to Haddow et al.Clin Infect Dis. 2015 May 1;60(9):1442-3. doi: 10.1093/cid/civ045. Epub 2015 Feb 2. Clin Infect Dis. 2015. PMID: 25645217 Free PMC article. No abstract available.
References
-
- Sevigny JJ, Albert SM, McDermott MP, et al. Evaluation of HIV RNA and markers of immune activation as predictors of HIV-associated dementia. Neurology. 2004;63:2084–90. - PubMed
-
- McArthur JC, Brew BJ. HIV-associated neurocognitive disorders: is there a hidden epidemic? AIDS. 2010;24:1367–70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
