

Comparison of risk and age at diagnosis of myocardial infarction, end-stage renal disease, and non-AIDS-defining cancer in HIV-infected versus uninfected adults
- PMID: 25362204
- PMCID: PMC4318916
- DOI: 10.1093/cid/ciu869
Comparison of risk and age at diagnosis of myocardial infarction, end-stage renal disease, and non-AIDS-defining cancer in HIV-infected versus uninfected adults
Abstract
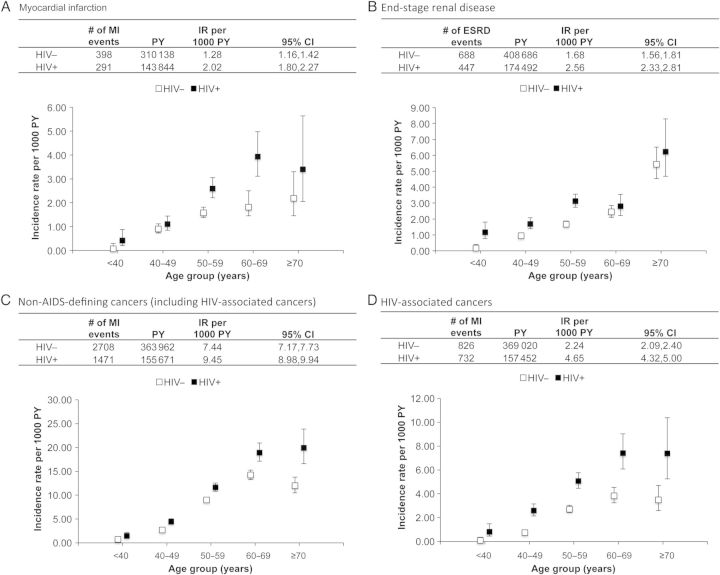
Background: Although it has been shown that human immunodeficiency virus (HIV)-infected adults are at greater risk for aging-associated events, it remains unclear as to whether these events happen at similar, or younger ages, in HIV-infected compared with uninfected adults. The objective of this study was to compare the median age at, and risk of, incident diagnosis of 3 age-associated diseases in HIV-infected and demographically similar uninfected adults.
Methods: The study was nested in the clinical prospective Veterans Aging Cohort Study of HIV-infected and demographically matched uninfected veterans, from 1 April 2003 to 31 December 2010. The outcomes were validated diagnoses of myocardial infarction (MI), end-stage renal disease (ESRD), and non-AIDS-defining cancer (NADC). Differences in mean age at, and risk of, diagnosis by HIV status were estimated using multivariate linear regression models and Cox proportional hazards models, respectively.
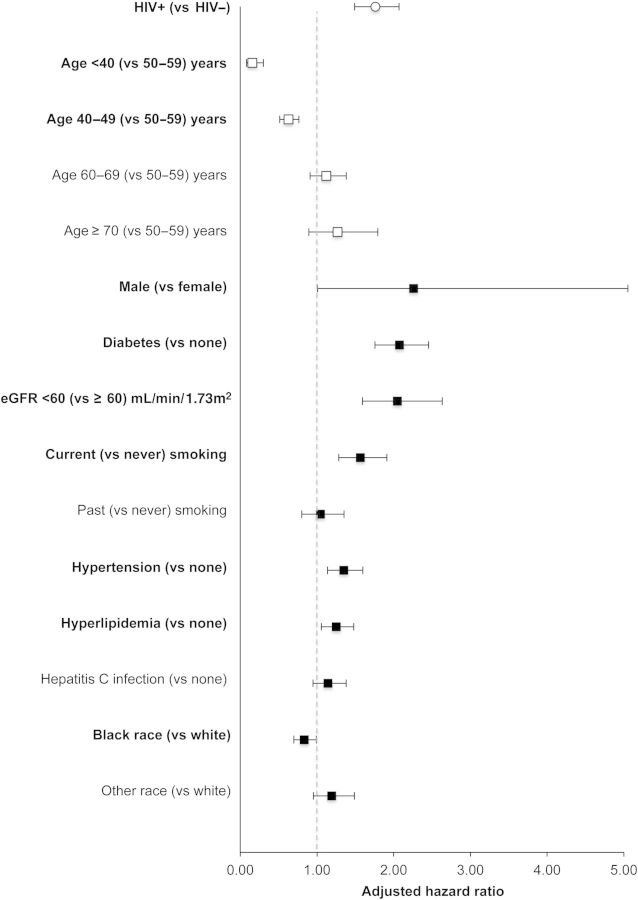
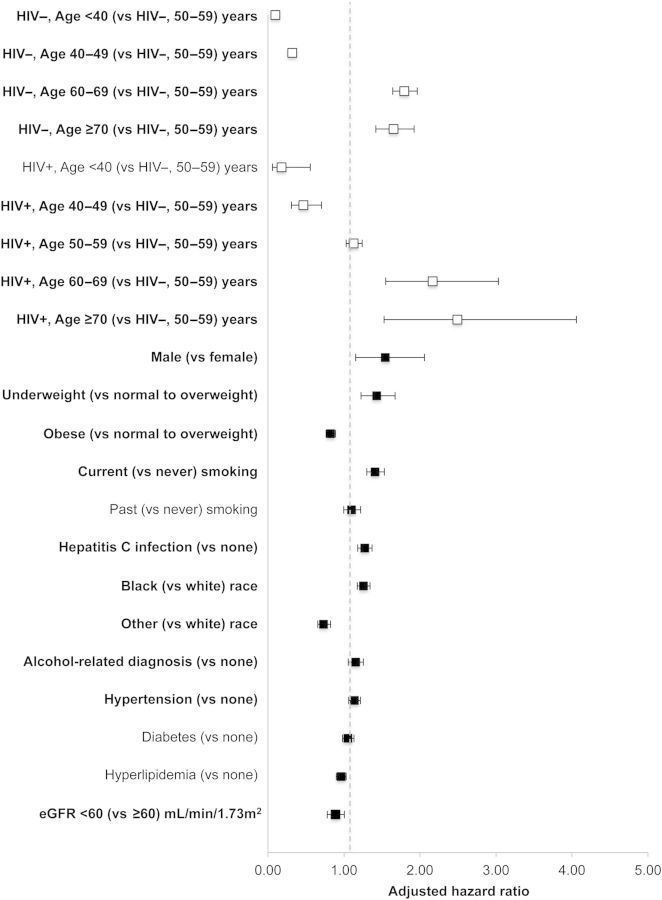
Results: A total of 98 687 (31% HIV-infected and 69% uninfected) adults contributed >450 000 person-years and 689 MI, 1135 ESRD, and 4179 NADC incident diagnoses. Mean age at MI (adjusted mean difference, -0.11; 95% confidence interval [CI], -.59 to .37 years) and NADC (adjusted mean difference, -0.10 [95% CI, -.30 to .10] years) did not differ by HIV status. HIV-infected adults were diagnosed with ESRD at an average age of 5.5 months younger than uninfected adults (adjusted mean difference, -0.46 [95% CI, -.86 to -.07] years). HIV-infected adults had a greater risk of all 3 outcomes compared with uninfected adults after accounting for important confounders.
Conclusions: HIV-infected adults had a higher risk of these age-associated events, but they occurred at similar ages than those without HIV.
Keywords: HIV infection; aging; end-stage renal disease; myocardial infarction; non-AIDS-defining cancers.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- May MT, Ingle SM. Life expectancy of HIV-positive adults: a review. Sexual Health. 2011;8:526–33. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–60. - PubMed
-
- The HIV and Aging Consensus Project. American Academy of HIV Medicine; Recommended treatment strategies for clinicians managing older patients with HIV. Available at: http://aahivm.org/Upload_Module/upload/HIV%20and%20Aging/Aging%20report%.... Accessed 20 October 2014.
-
- Martin J, Volberding P. HIV and premature aging: a field still in its infancy. Ann Intern Med. 2010;153:477–9. - PubMed
Publication types
MeSH terms
Grants and funding
- U24 AA022001/AA/NIAAA NIH HHS/United States
- R01-HL095136/HL/NHLBI NIH HHS/United States
- P30 MH062294/MH/NIMH NIH HHS/United States
- U24 AA022007/AA/NIAAA NIH HHS/United States
- R01 HS018372/HS/AHRQ HHS/United States
- R01-HL090342/HL/NHLBI NIH HHS/United States
- U10 AA013566/AA/NIAAA NIH HHS/United States
- U13 AA022864/AA/NIAAA NIH HHS/United States
- U01 AA020799/AA/NIAAA NIH HHS/United States
- U01-AA020795/AA/NIAAA NIH HHS/United States
- K01-AI093197/AI/NIAID NIH HHS/United States
- R01 HL095136/HL/NHLBI NIH HHS/United States
- R01 DA035616/DA/NIDA NIH HHS/United States
- F31 CA180775/CA/NCI NIH HHS/United States
- R01 HL090342/HL/NHLBI NIH HHS/United States
- T32 MH020031/MH/NIMH NIH HHS/United States
- U01 AA020795/AA/NIAAA NIH HHS/United States
- P01-DK056492/DK/NIDDK NIH HHS/United States
- R01 CA173754/CA/NCI NIH HHS/United States
- R01-HS018372/HS/AHRQ HHS/United States
- P30-MH062294/MH/NIMH NIH HHS/United States
- I01 RX000667/RX/RRD VA/United States
- F31-CA180775/CA/NCI NIH HHS/United States
- P01 DK056492/DK/NIDDK NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- U24-AA022001/AA/NIAAA NIH HHS/United States
- U01-AA020799/AA/NIAAA NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- U01-AA020790/AA/NIAAA NIH HHS/United States
- U01-A1069918/PHS HHS/United States
- R01DA035616/DA/NIDA NIH HHS/United States
- U24-AA020794/AA/NIAAA NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
