

Altered in vitro endothelial repair and monocyte migration in obstructive sleep apnea: implication of VEGF and CRP
- PMID: 25364078
- PMCID: PMC4196066
- DOI: 10.5665/sleep.4180
Altered in vitro endothelial repair and monocyte migration in obstructive sleep apnea: implication of VEGF and CRP
Abstract
Study objectives: Although obstructive sleep apnea (OSA) causes cardiovascular morbidities through atherosclerosis induced by inflammation and endothelial dysfunction, OSA patients exhibit elevated plasma vascular endothelial growth factor (VEGF), which may represent an adaptive response to intermittent hypoxia. The aims of this study were to investigate whether in vitro endothelial wound healing and monocyte migration are affected by patient serum, and to determine the implication of circulating factors (VEGF and C-reactive protein).
Patients: Serum was collected from healthy controls (HC), "healthy" OSA, and metabolic syndrome (MS) patients with or without OSA.
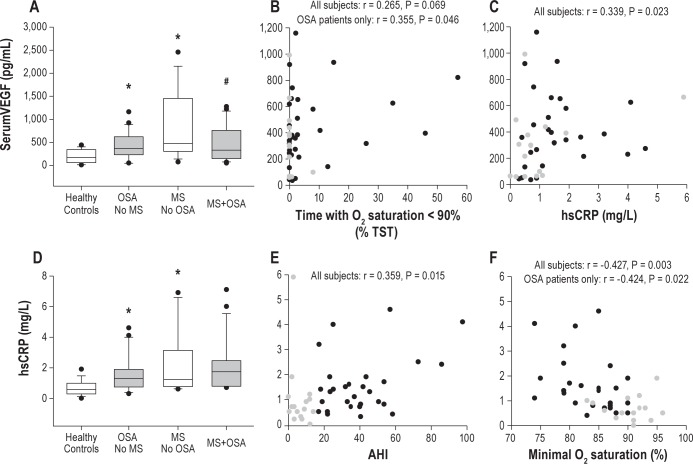
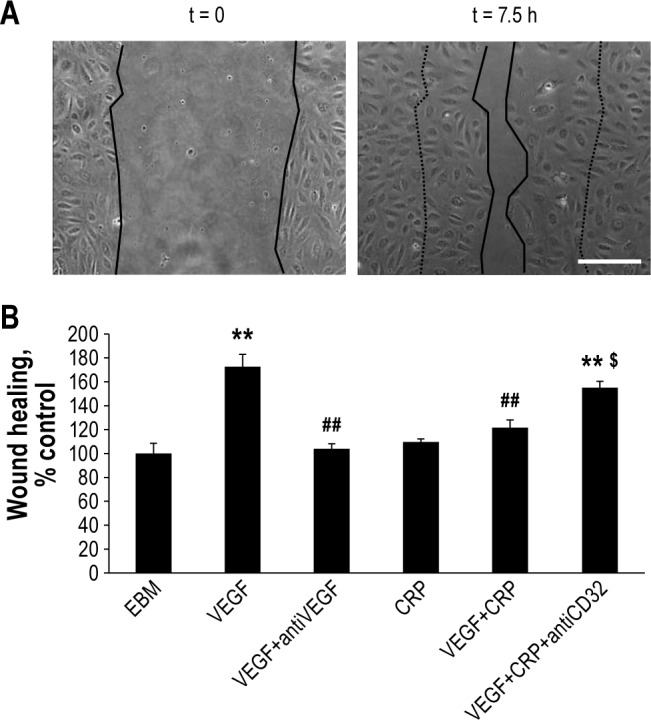
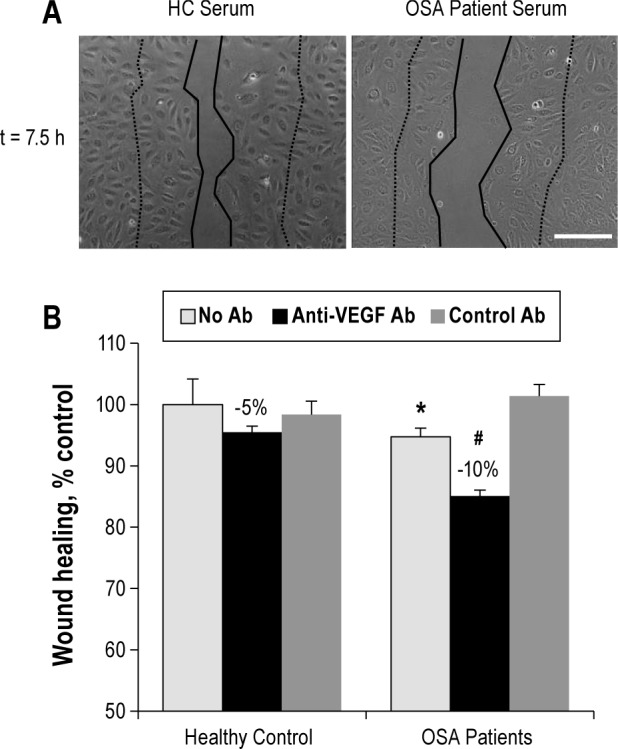
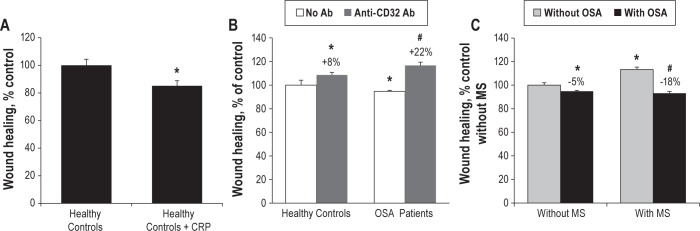
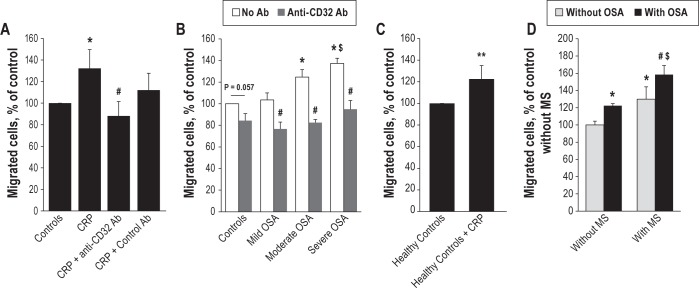
Measurements and results: Along with the presence of OSA and/or MS, both VEGF and hsCRP were significantly elevated in patient serum. Their specific role was tested with blocking antibodies on primary endothelial cells for wound healing assay and on human monocytes for migration assay. Endothelial wound healing was reduced with OSA compared to HC serum, and even more significantly using MS+OSA patient serum. Altered wound healing with OSA serum was unmasked when blocking VEGF and restored when blocking CRP. Monocyte migration was activated with OSA serum, and further enhanced by MS+OSA patient serum. Blocking CRP in serum inhibited this migration.
Conclusions: Serum from OSA patient alters in vitro endothelial cell repair function and activates monocyte migration; this is further aggravated with the presence of metabolic syndrome. These effects are partly driven by VEGF and CRP, suggesting an unfavorable balance between the pro healing (VEGF) and pro injury (CRP) factors that may promote vascular injury in OSA with and without metabolic syndrome.
Keywords: VEGF; endothelial repair; hsCRP; metabolic syndrome; obstructive sleep apnea.
Figures
Similar articles
-
Impact of OSA on biological markers in morbid obesity and metabolic syndrome.J Clin Sleep Med. 2014 Mar 15;10(3):263-70. doi: 10.5664/jcsm.3524. J Clin Sleep Med. 2014. PMID: 24634623 Free PMC article.
-
Circadian variability of fibrinolytic markers and endothelial function in patients with obstructive sleep apnea.Sleep. 2014 Feb 1;37(2):359-67. doi: 10.5665/sleep.3414. Sleep. 2014. PMID: 24497664 Free PMC article.
-
Serum levels of vascular endothelial growth factor are elevated in patients with obstructive sleep apnea and severe nighttime hypoxia.Am J Respir Crit Care Med. 2002 Jan 1;165(1):67-70. doi: 10.1164/ajrccm.165.1.2101062. Am J Respir Crit Care Med. 2002. PMID: 11779732
-
Obstructive sleep apnea syndrome, vascular pathology, endothelial function and endothelial cells and circulating microparticles.Arch Med Res. 2013 Aug;44(6):409-14. doi: 10.1016/j.arcmed.2013.08.005. Epub 2013 Sep 17. Arch Med Res. 2013. PMID: 24051041 Review.
-
Impact of continuous positive airway pressure on vascular endothelial growth factor in patients with obstructive sleep apnea: a meta-analysis.Sleep Breath. 2019 Mar;23(1):5-12. doi: 10.1007/s11325-018-1660-4. Epub 2018 Apr 18. Sleep Breath. 2019. PMID: 29671205 Review.
Cited by
-
Obstructive sleep apnea: a major risk factor for COVID-19 encephalopathy?BMC Neurol. 2023 Sep 27;23(1):340. doi: 10.1186/s12883-023-03393-2. BMC Neurol. 2023. PMID: 37752429 Free PMC article.
-
Intermittent Hypoxia Is Associated With High Hypoxia Inducible Factor-1α but Not High Vascular Endothelial Growth Factor Cell Expression in Tumors of Cutaneous Melanoma Patients.Front Neurol. 2018 Apr 26;9:272. doi: 10.3389/fneur.2018.00272. eCollection 2018. Front Neurol. 2018. PMID: 29755400 Free PMC article.
-
Serum from obstructive sleep apnea patients induces inflammatory responses in coronary artery endothelial cells.Atherosclerosis. 2016 Nov;254:59-66. doi: 10.1016/j.atherosclerosis.2016.09.017. Epub 2016 Sep 22. Atherosclerosis. 2016. PMID: 27693879 Free PMC article.
-
The link between the sphingolipid rheostat and obstructive sleep apnea.Sci Rep. 2023 May 11;13(1):7675. doi: 10.1038/s41598-023-34717-4. Sci Rep. 2023. PMID: 37169814 Free PMC article.
-
Circulating microRNAs and endothelial cell migration rate are associated with metabolic syndrome and fitness level in postmenopausal African American women.Physiol Rep. 2019 Jul;7(14):e14173. doi: 10.14814/phy2.14173. Physiol Rep. 2019. PMID: 31347282 Free PMC article.
References
-
- Baguet JP, Barone-Rochette G, Tamisier R, Levy P, Pepin JL. Mechanisms of cardiac dysfunction in obstructive sleep apnea. Nat Rev Cardiol. 2010;9:679–88. - PubMed
-
- Levy P, Pepin JL, Arnaud C, et al. Intermittent hypoxia and sleep-disordered breathing: current concepts and perspectives. Eur Respir J. 2008;32:1082–95. - PubMed
-
- Levy P, Pepin JL, Arnaud C, Baguet JP, Dematteis M, Mach F. Obstructive sleep apnea and atherosclerosis. Prog Cardiovasc Dis. 2009;51:400–10. - PubMed
-
- McNicholas WT. Obstructive sleep apnea and inflammation. Prog Cardiovasc Dis. 2009;51:392–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
