

To the occiput or not? C1-c2 ligamentous laxity in children with down syndrome
- PMID: 25364324
- PMCID: PMC4212581
- DOI: 10.1055/s-0034-1386749
To the occiput or not? C1-c2 ligamentous laxity in children with down syndrome
Abstract
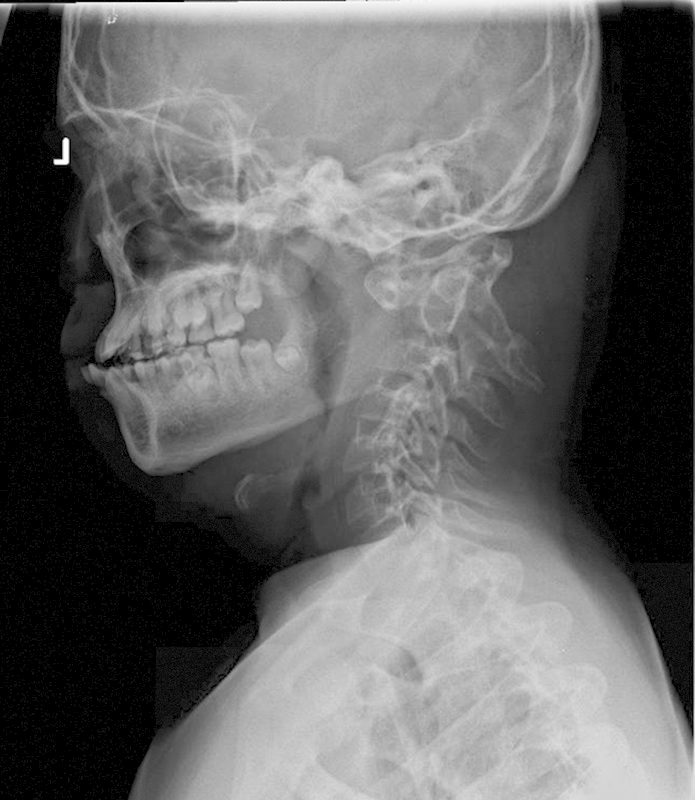
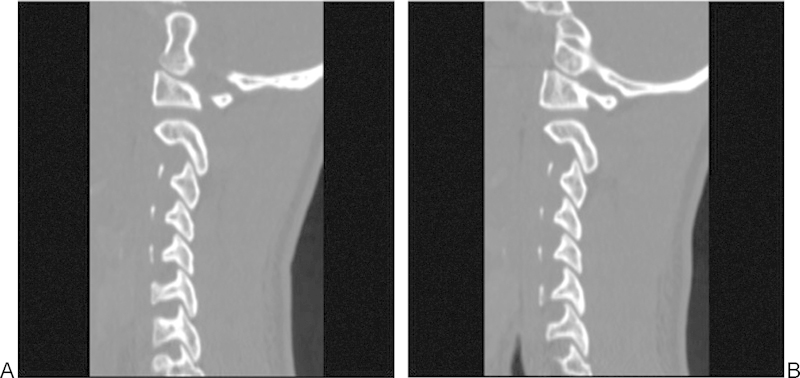
Study Design Retrospective case review. Objective Atlantoaxial instability with and without basilar invagination poses a considerable challenge in management regarding reduction, surgical approach, decompression, instrumentation choice, and extent of fusion. A variety of strategies have been described to reduce and stabilize cranial settling with basilar invagination. Modern instrumentation options included extension to the occiput, C1-C2 transarticular fixation, and C1 lateral mass-C2 pars among others. Since not all cases of cranial settling are the same, their treatment strategies also differ. Factors such as local vascular anatomy, amount of subluxation, need for distraction, and shape of occipital condyles will dictate level and type of instrumentation. The objective of this study was to outline treatment options and provide a rationale for the surgical plan. Methods Two cases of C1-C2 instability in patients with Down syndrome are described. Case 2 underwent C1-C2 instrumented fusion, whereas case 1 involved posterior instrumented fusion to the occiput. Results Both patients tolerated the procedures well. There were no complications. Minimum follow-up was 1 year. There was no loss of reduction. Solid arthrodesis was achieved in both cases. Conclusion Successful reduction can be achieved with both C1-C2 instrumented fusion as well as O-C instrument fusion. Factors such as local vascular anatomy, amount of subluxation, need for distraction, and shape of occipital condyles will dictate level and type of instrumentation.
Keywords: C1–C2 instability; Down syndrome; basilar invagination; occiput; os odontoideum; pediatric.
Conflict of interest statement
Figures








Similar articles
-
Fusions at the craniovertebral junction.Childs Nerv Syst. 2008 Oct;24(10):1209-24. doi: 10.1007/s00381-008-0607-7. Epub 2008 Apr 4. Childs Nerv Syst. 2008. PMID: 18389260 Review.
-
Single-stage anterior release and posterior instrumented fusion for irreducible atlantoaxial dislocation with basilar invagination.Spine J. 2016 Jan 1;16(1):1-9. doi: 10.1016/j.spinee.2015.09.037. Epub 2015 Sep 26. Spine J. 2016. PMID: 26409417
-
Occiput/C1-C2 fixations using intra-laminar screw of axis - A long-term follow-up.Br J Neurosurg. 2015 Apr;29(2):260-4. doi: 10.3109/02688697.2014.987211. Epub 2014 Dec 4. Br J Neurosurg. 2015. PMID: 25472926
-
Occipitocervical or C1-C2 fusion using allograft bone in pediatric patients with Down syndrome 8 years of age or younger.J Pediatr Orthop B. 2019 Jul;28(4):405-410. doi: 10.1097/BPB.0000000000000622. J Pediatr Orthop B. 2019. PMID: 30855547
-
Temporary fusionless posterior occipitocervical fixation for a proximal junctional type II odontoid fracture after previous C2-pelvis fusion: case report, description of a new surgical technique, and review of the literature.Eur Spine J. 2017 May;26(Suppl 1):243-248. doi: 10.1007/s00586-017-5093-8. Epub 2017 Apr 13. Eur Spine J. 2017. PMID: 28409288 Review.
References
-
- Abumi K, Takada T, Shono Y, Kaneda K, Fujiya M. Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine (Phila Pa 1976) 1999;24(14):1425–1434. - PubMed
-
- Goel A, Bhatjiwale M, Desai K. Basilar invagination: a study based on 190 surgically treated patients. J Neurosurg. 1998;88(6):962–968. - PubMed
-
- Bhangoo R S, Crockard H A. Transmaxillary anterior decompressions in patients with severe basilar impression. Clin Orthop Relat Res. 1999;(359):115–125. - PubMed
-
- Botelho R V, Neto E B, Patriota G C, Daniel J W, Dumont P A, Rotta J M. Basilar invagination: craniocervical instability treated with cervical traction and occipitocervical fixation. Case report. J Neurosurg Spine. 2007;7(4):444–449. - PubMed
-
- Simsek S Yigitkanli K Belen D Bavbek M Halo traction in basilar invagination: technical case report Surg Neurol 2006663311–314., discussion 314 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
