

Impact of high prevalence of pseudomonas and polymicrobial gram-negative infections in major sub-/total traumatic amputations on empiric antimicrobial therapy: a retrospective study
- PMID: 25364376
- PMCID: PMC4216372
- DOI: 10.1186/1749-7922-9-55
Impact of high prevalence of pseudomonas and polymicrobial gram-negative infections in major sub-/total traumatic amputations on empiric antimicrobial therapy: a retrospective study
Abstract
Introduction: Emergency treatment of major sub-/total traumatic amputations continue to represent a clinical challenge due to high infection rates and serious handicaps. Effective treatment is based on two columns: surgery and antimicrobial therapy. Detailed identification of pathogen spectrum and epidemiology associated with these injuries is of tremendous importance as it guides the initial empiric antibiotic regimen and prevents adverse septic effents.
Methods: In this retrospective study 51 patients with major traumatic amputations (n = 16) and subtotal amputations (n = 35) treated from 2001 to 2010 in our trauma center were investigated. All patients received emergency surgery, debridement with microbiological testing within 6 h after admission and empircic antimicrobial therapy. Additionally to baseline patient characteristics, the incidence of positive standardized microbiologic testing combined with clinical signs of infection, pathogen spectrum, administered antimicrobial agents and clinical complications were analyzed.
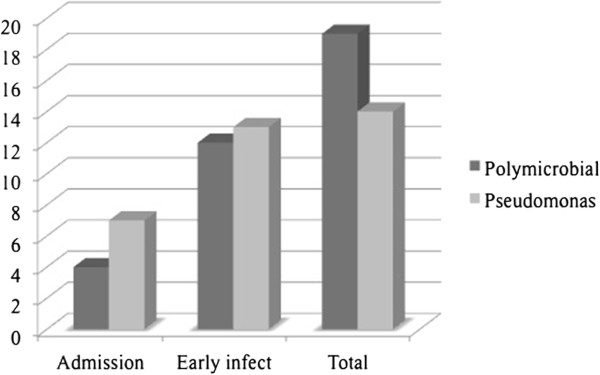
Results: 70.6% of the patients (n = 36) acquired wound infection. In 39% wounds were contaminated on day 1, whereas the mean length of duration until first pathogen detection was 9.1 ± 13.4 days after injury. In 37% polymicrobial colonization and 28% Pseudomonas were responsible for wound infections during hospitalization. In 45% the empirc antimicrobial therapy focussed on Gram positive strains did not cover the detected bacteria, according antimicrobial resistogram. It was significantly more often found in infections associated with Pseudomonas (p 0.02) or polymicrobial wound infections.
Conclusions: This epidemiologic study reveals a pathogen shift from Gram-positive to Gram-negative strains with high incidence of Pseudomonas and polymicrobial infections in sub-/total major traumatic amputations. Therefore, empiric antimicrobial treatment historically focussing on Gram-positive strains must be adjusted. We recommend the use of Piperacillin/Tazobactam for these injuries. As soon as possible antimicrobial treatment should be changed from empiric to goal directed therapy according to the microbiological tests and resistogram results.
Keywords: Amputation; Antimicrobial therapy; Infection; Open fracture; Pathogen; Pseudomonas; Trauma.
Figures

References
-
- Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453–458. - PubMed
-
- Tscherne H, Oestern HJ. [A new classification of soft-tissue damage in open and closed fractures (author's transl)] Unfallheilkunde. 1982;85(3):111–115. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
