

Risk of bleeding with dabigatran in atrial fibrillation
- PMID: 25365537
- PMCID: PMC6608584
- DOI: 10.1001/jamainternmed.2014.5398
Risk of bleeding with dabigatran in atrial fibrillation
Erratum in
-
Errors in Figures.JAMA Intern Med. 2018 Dec 1;178(12):1732. doi: 10.1001/jamainternmed.2018.5747. JAMA Intern Med. 2018. PMID: 30357258 Free PMC article. No abstract available.
Abstract
Importance: It remains unclear whether dabigatran etexilate mesylate is associated with higher risk of bleeding than warfarin sodium in real-world clinical practice.
Objective: To compare the risk of bleeding associated with dabigatran and warfarin using Medicare data.
Design, setting, and participants: In this retrospective cohort study, we used pharmacy and medical claims in 2010 to 2011 from a 5% random sample of Medicare beneficiaries. We identified participants as those newly diagnosed as having atrial fibrillation from October 1, 2010, through October 31, 2011, and who initiated dabigatran or warfarin treatment within 60 days of initial diagnosis. We followed up patients until discontinued use or switch of anticoagulants, death, or December 31, 2011.
Exposures: Dabigatran users (n = 1302) and warfarin users (n = 8102).
Main outcomes and measures: We identified any bleeding events and categorized them as major and minor bleeding by anatomical site. Major bleeding events included intracranial hemorrhage, hemoperitoneum, and inpatient or emergency department stays for hematuria, gastrointestinal, or other hemorrhage. We used a propensity score weighting mechanism to balance patient characteristics between 2 groups and Cox proportional hazards regression models to evaluate the risk of bleeding. We further examined the risk of bleeding for 4 subgroups of high-risk patients: those 75 years or older, African Americans, those with chronic kidney disease, and those with more than 7 concomitant comorbidities.
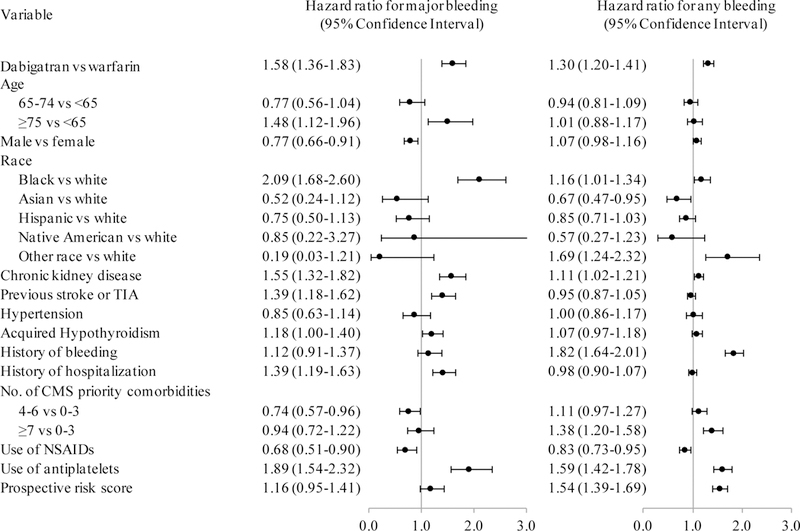
Results: Dabigatran was associated with a higher risk of bleeding relative to warfarin, with hazard ratios of 1.30 (95% CI, 1.20-1.41) for any bleeding event, 1.58 (95% CI, 1.36-1.83) for major bleeding, and 1.85 (95% CI, 1.64-2.07) for gastrointestinal bleeding. The risk of intracranial hemorrhage was higher among warfarin users, with a hazard ratio of 0.32 (95% CI, 0.20-0.50) for dabigatran compared with warfarin. Dabigatran was consistently associated with an increased risk of major bleeding and gastrointestinal hemorrhage for all subgroups analyzed. The risk of major bleeding among dabigatran users was especially high for African Americans and patients with chronic kidney disease.
Conclusions and relevance: Dabigatran was associated with a higher incidence of major bleeding (regardless of the anatomical site), a higher risk of gastrointestinal bleeding, but a lower risk of intracranial hemorrhage. Thus, dabigatran should be prescribed with caution, especially among high-risk patients.
Conflict of interest statement
Figures


Comment in
-
The importance of postapproval data for dabigatran.JAMA Intern Med. 2015 Jan;175(1):25. doi: 10.1001/jamainternmed.2014.6265. JAMA Intern Med. 2015. PMID: 25365377 No abstract available.
-
Atrial fibrillation: Risk of bleeding with dabigatran versus warfarin particularly high in CKD.Nat Rev Nephrol. 2015 Jan;11(1):3. doi: 10.1038/nrneph.2014.221. Epub 2014 Nov 25. Nat Rev Nephrol. 2015. PMID: 25421829 No abstract available.
-
Gastrointestinal bleeding. Gastrointestinal bleeding risk is increased by novel anticoagulants.Nat Rev Gastroenterol Hepatol. 2015 Mar;12(3):131-2. doi: 10.1038/nrgastro.2015.7. Epub 2015 Jan 20. Nat Rev Gastroenterol Hepatol. 2015. PMID: 25601661
-
[Dabigatran and risk of bleeding].Praxis (Bern 1994). 2015 Jan 28;104(3):157-8. doi: 10.1024/1661-8157/a001908. Praxis (Bern 1994). 2015. PMID: 25626386 German. No abstract available.
-
One-Year Risk of Bleeding With Dabigatran in Patients With Atrial Fibrillation: Placing Real-World Results Into Perspective.JAMA Intern Med. 2015 Jul;175(7):1242-3. doi: 10.1001/jamainternmed.2015.1271. JAMA Intern Med. 2015. PMID: 26146916 No abstract available.
-
Bleeding in Patients of African Ancestry Using Dabigatran: A Potential Effect of Creatine Kinase.JAMA Intern Med. 2015 Jul;175(7):1243. doi: 10.1001/jamainternmed.2015.1274. JAMA Intern Med. 2015. PMID: 26146917 No abstract available.
-
The Role of Selection in the Risk of Bleeding With Dabigatran in Patients With Atrial Fibrillation.JAMA Intern Med. 2015 Jul;175(7):1243-4. doi: 10.1001/jamainternmed.2015.1277. JAMA Intern Med. 2015. PMID: 26146918 No abstract available.
-
A Methodological Appraisal of Recent Real-World Data Publications on Dabigatran.JAMA Intern Med. 2015 Jul;175(7):1244. doi: 10.1001/jamainternmed.2015.1280. JAMA Intern Med. 2015. PMID: 26146919 No abstract available.
-
Dosage of Dabigatran as a Risk Factor for Bleeding in Atrial Fibrillation.JAMA Intern Med. 2015 Jul;175(7):1244-5. doi: 10.1001/jamainternmed.2015.1286. JAMA Intern Med. 2015. PMID: 26146920 No abstract available.
-
Patient Characteristics and Risk of Bleeding With Dabigatran in Atrial Fibrillation.JAMA Intern Med. 2015 Jul;175(7):1245. doi: 10.1001/jamainternmed.2015.1289. JAMA Intern Med. 2015. PMID: 26146921 No abstract available.
-
Risk of Bleeding With Dabigatran in 2010-2011 Medicare Data.JAMA Intern Med. 2015 Jul;175(7):1245-7. doi: 10.1001/jamainternmed.2015.1299. JAMA Intern Med. 2015. PMID: 26146922 Free PMC article. No abstract available.
References
-
- Summary review for new drug application - dabigatran etexilate. 2010; http://www.accessdata.fda.gov/drugsatfda_docs/nda/2010/0225120rig1s000Su... Accessed October 3, 2013.
-
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12): 1139–1151. - PubMed
-
- Cano EL, Miyares MA. Clinical challenges in a patient with dabigatran-induced fatal hemorrhage. Am J Geriatr Pharmacother. 2012;10(2):160–163. - PubMed
-
- Chen BC, Viny AD, Garlich FM, et al. Hemorrhagic complications associated with dabigatran use. Clin Toxicol. 2012;50(9):854–857. - PubMed
-
- Bene J, Said W, Rannou M, Deheul S, Coupe P, Gautier S. Rectal bleeding and hemostatic disorders induced by dabigatran etexilate in 2 elderly patients. Ann Pharmacother. 2012;46(6):5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
