

Hospital-based acute care use in survivors of septic shock
- PMID: 25365724
- PMCID: PMC4359663
- DOI: 10.1097/CCM.0000000000000693
Hospital-based acute care use in survivors of septic shock
Abstract
Objectives: Septic shock is associated with increased long-term morbidity and mortality. However, little is known about the use of hospital-based acute care in survivors after hospital discharge. The objectives of the study were to examine the frequency, timing, causes, and risk factors associated with emergency department visits and hospital readmissions within 30 days of discharge.
Design: Retrospective cohort study.
Setting: Tertiary, academic hospital in the United States.
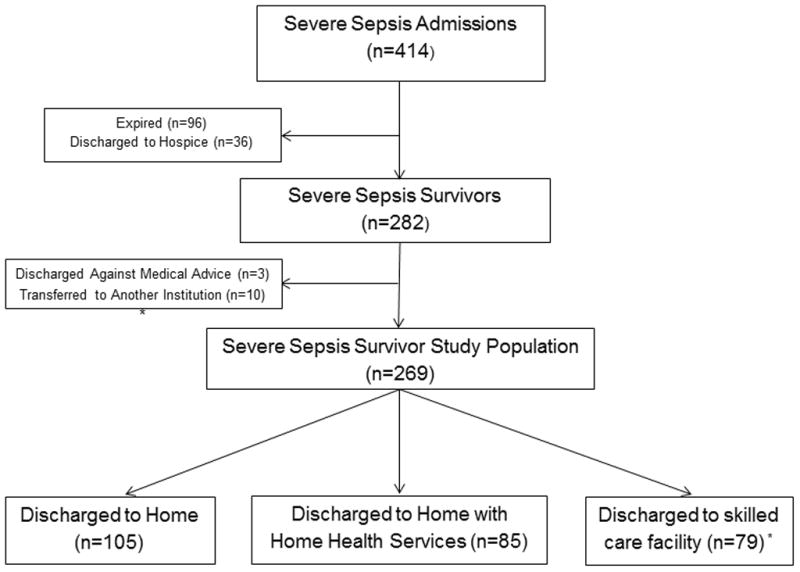
Patients: Patients admitted with septic shock (serum lactate≥4 mmol/L or refractory hypotension) and discharged alive to a nonhospice setting between 2007 and 2010.
Interventions: None.
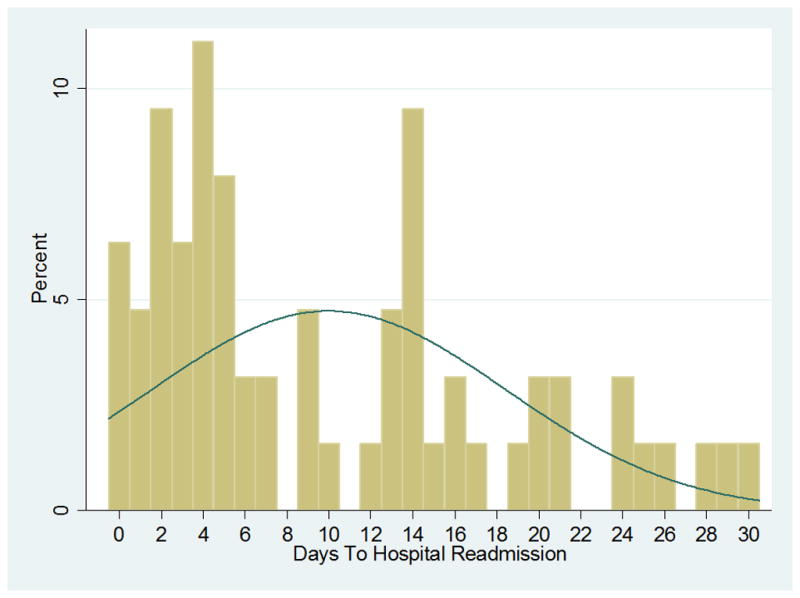
Measurements and main results: The coprimary outcomes were all-cause hospital readmission and emergency department visits (treat-and-release encounters) within 30 days to any of the three health system hospitals. Of 269 at-risk survivors, 63 (23.4%; 95% CI, 18.2-28.5) were readmitted within 30 days of discharge and another 12 (4.5%; 95% CI, 2.3-7.7) returned to the emergency department for a treat-and-release visit. Readmissions occurred within 15 days of discharge in 75% of cases and were more likely in oncology patients (p=0.001) and patients with a longer hospital length of stay (p=0.04). Readmissions were frequently due to another life-threatening condition and resulted in death or discharge to hospice in 16% of cases. The reasons for readmission were deemed potentially related to the index septic shock hospitalization in 78% (49 of 63) of cases. The most common cause was infection related, accounting for 46% of all 30-day readmissions, followed by cardiovascular or thromboembolic events (18%).
Conclusions: The use of hospital-based acute care appeared to be common in septic shock survivors. Encounters often led to readmission within 15 days of discharge, were frequently due to another acute condition, and appeared to result in substantial morbidity and mortality. Given the potential public health implications of these findings, validation studies are needed.
Conflict of interest statement
Figures
Comment in
-
How much more intelligent do we have to be about the burden of severe sepsis and septic shock?Crit Care Med. 2015 Apr;43(4):906-7. doi: 10.1097/CCM.0000000000000903. Crit Care Med. 2015. PMID: 25768351 No abstract available.
References
-
- Gaieski DF, Edwards JM, Kallan MJ, et al. Benchmarking the Incidence and Mortality of Severe Sepsis in the United States. Crit Care Med. 2013;41:1167–74. - PubMed
-
- Lagu T, Rothberg MB, Shieh MS, et al. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40:754–761. - PubMed
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–1377. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
