

Interoceptive dysfunction: toward an integrated framework for understanding somatic and affective disturbance in depression
- PMID: 25365763
- PMCID: PMC4346391
- DOI: 10.1037/a0038101
Interoceptive dysfunction: toward an integrated framework for understanding somatic and affective disturbance in depression
Abstract
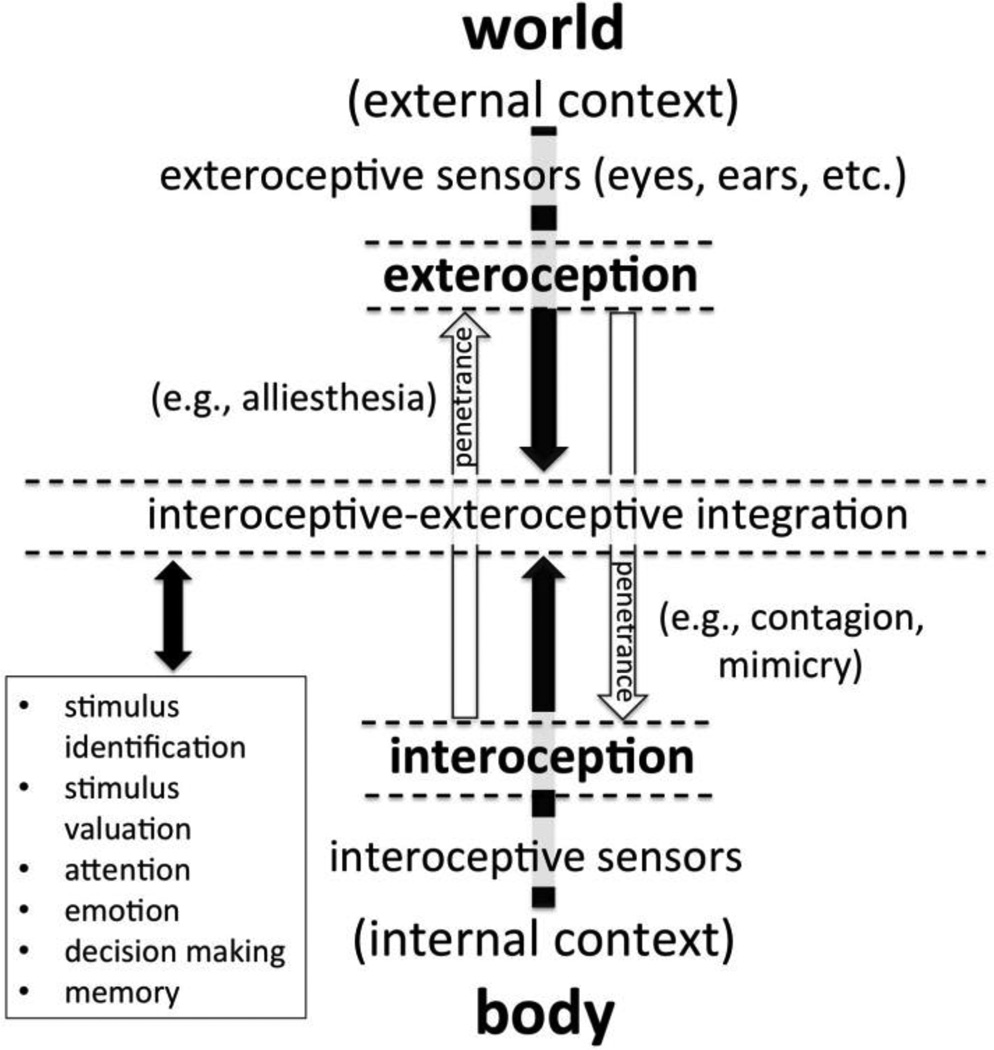
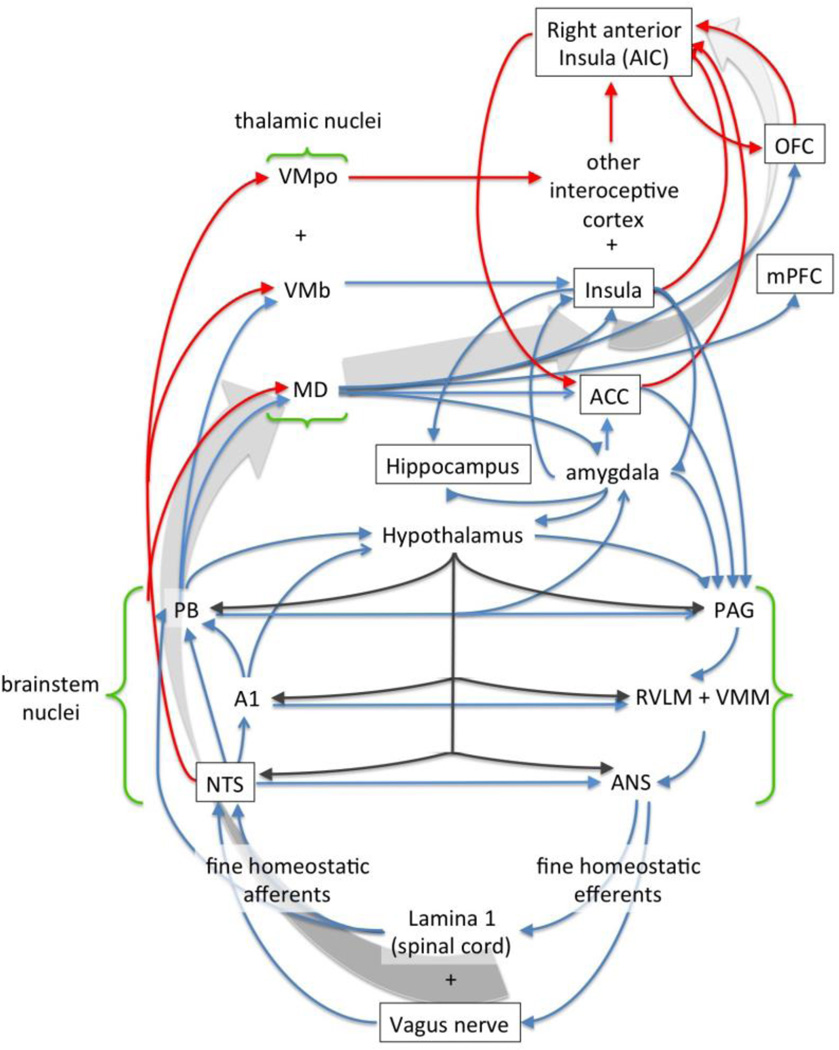
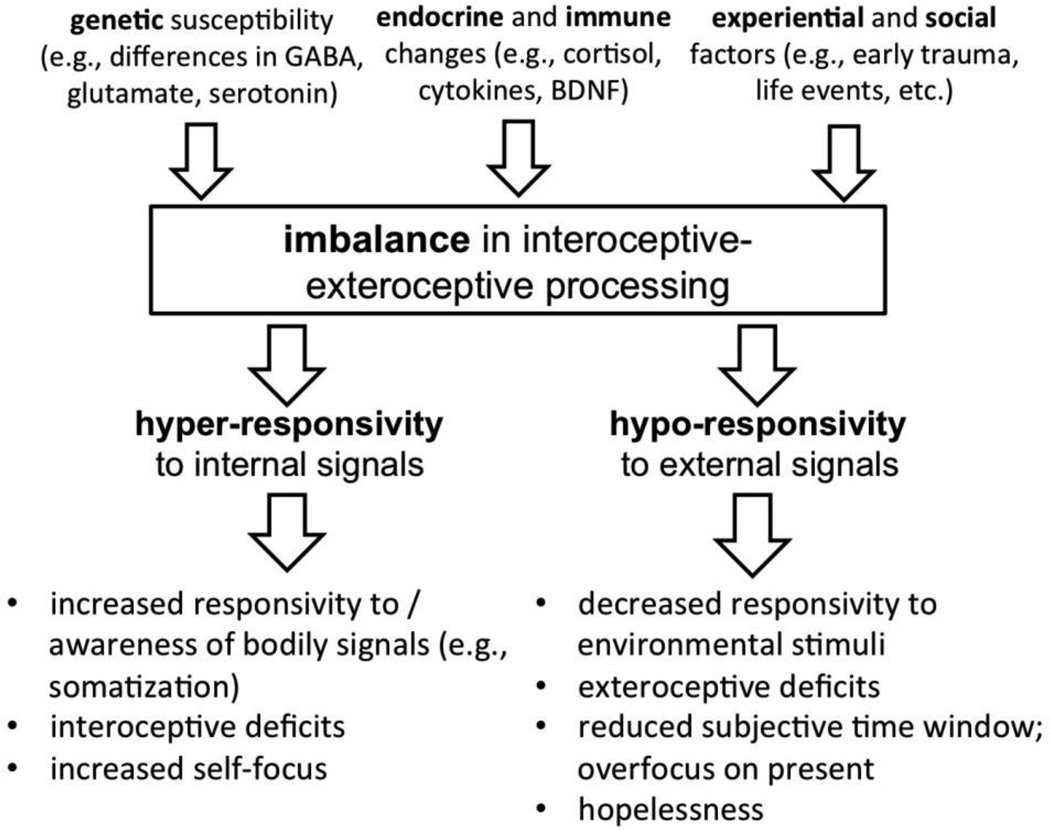
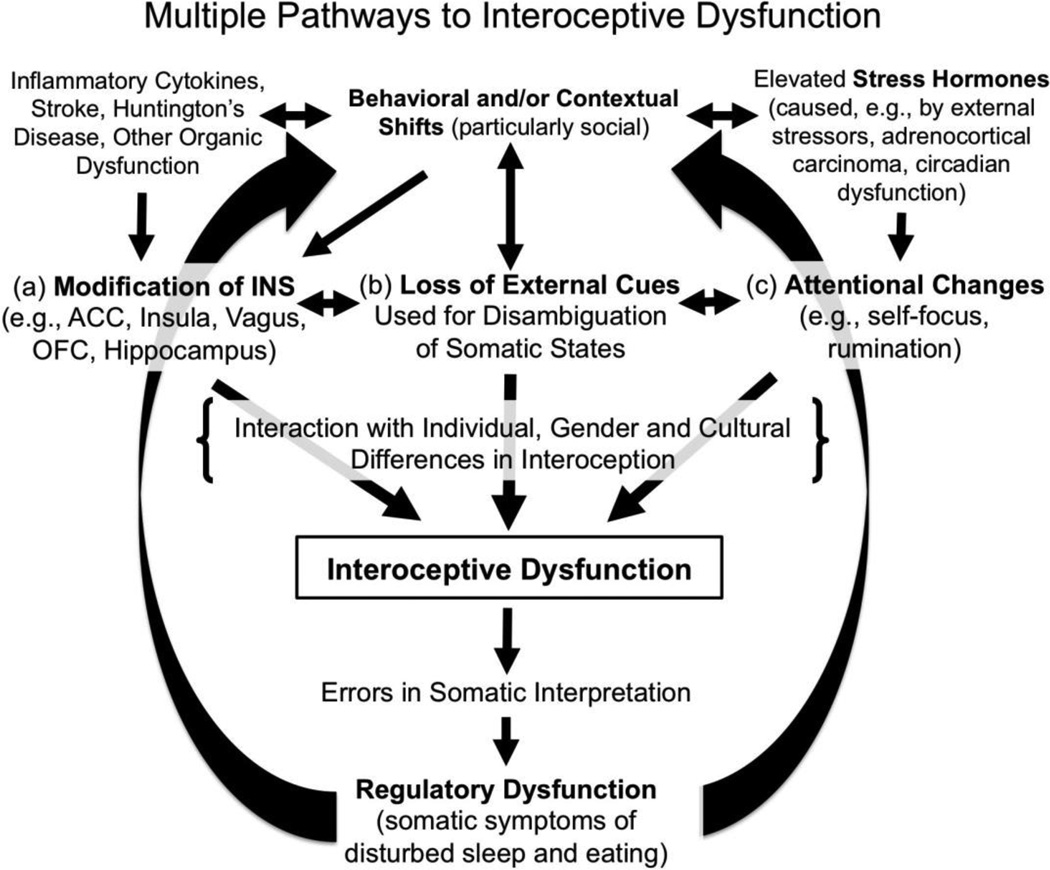
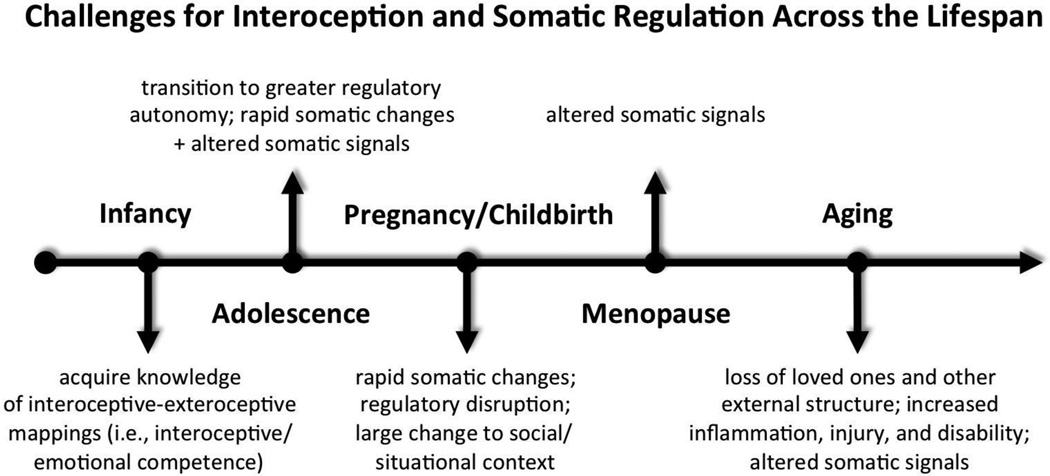
Depression is characterized by disturbed sleep and eating, a variety of other nonspecific somatic symptoms, and significant somatic comorbidities. Why there is such close association between cognitive and somatic dysfunction in depression is nonetheless poorly understood. An explosion of research in the area of interoception-the perception and interpretation of bodily signals-over the last decade nonetheless holds promise for illuminating what have until now been obscure links between the social, cognitive-affective, and somatic features of depression. This article reviews rapidly accumulating evidence that both somatic signaling and interoception are frequently altered in depression. This includes comparative studies showing vagus-mediated effects on depression-like behaviors in rodent models as well as studies in humans indicating both dysfunction in the neural substrates for interoception (e.g., vagus, insula, anterior cingulate cortex) and reduced sensitivity to bodily stimuli in depression. An integrative framework for organizing and interpreting this evidence is put forward which incorporates (a) multiple potential pathways to interoceptive dysfunction; (b) interaction with individual, gender, and cultural differences in interoception; and (c) a developmental psychobiological systems perspective, emphasizing likely differential susceptibility to somatic and interoceptive dysfunction across the lifespan. Combined with current theory and evidence, it is suggested that core symptoms of depression (e.g., anhedonia, social deficits) may be products of disturbed interoceptive-exteroceptive integration. More research is nonetheless needed to fully elucidate the relationship between mind, body, and social context in depression.
PsycINFO Database Record (c) 2015 APA, all rights reserved.
Figures
Similar articles
-
Interoception, somatic symptoms, and somatization tendency in Chinese individuals with subsyndromal depression: A follow-up study.Psych J. 2024 Aug;13(4):616-624. doi: 10.1002/pchj.739. Epub 2024 Feb 16. Psych J. 2024. PMID: 38363643 Free PMC article.
-
A cross-sectional study on the relationship between interoceptive sensitivity and somatic symptoms in young bipolar disorder patients.BMC Psychiatry. 2025 Apr 9;25(1):355. doi: 10.1186/s12888-025-06801-8. BMC Psychiatry. 2025. PMID: 40205379 Free PMC article.
-
The Neural Bases of Interoceptive Encoding and Recall in Healthy Adults and Adults With Depression.Biol Psychiatry Cogn Neurosci Neuroimaging. 2018 Jun;3(6):546-554. doi: 10.1016/j.bpsc.2018.03.010. Epub 2018 Mar 27. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018. PMID: 29724684 Free PMC article.
-
Common threads: Altered interoceptive processes across affective and anxiety disorders.J Affect Disord. 2025 Jan 15;369:244-254. doi: 10.1016/j.jad.2024.09.135. Epub 2024 Sep 23. J Affect Disord. 2025. PMID: 39321982 Review.
-
The neurobiology of interoception in health and disease.Ann N Y Acad Sci. 2018 Sep;1428(1):112-128. doi: 10.1111/nyas.13915. Epub 2018 Jul 5. Ann N Y Acad Sci. 2018. PMID: 29974959 Review.
Cited by
-
Beyond Gender: Interoceptive Sensibility as a Key Predictor of Body Image Disturbances.Behav Sci (Basel). 2023 Dec 28;14(1):25. doi: 10.3390/bs14010025. Behav Sci (Basel). 2023. PMID: 38247677 Free PMC article.
-
Editorial: Embodying the Self: Neurophysiological Perspectives on the Psychopathology of Anomalous Bodily Experiences.Front Hum Neurosci. 2017 Dec 19;11:631. doi: 10.3389/fnhum.2017.00631. eCollection 2017. Front Hum Neurosci. 2017. PMID: 29311881 Free PMC article. No abstract available.
-
Interoception and Inflammation in Psychiatric Disorders.Biol Psychiatry Cogn Neurosci Neuroimaging. 2018 Jun;3(6):514-524. doi: 10.1016/j.bpsc.2017.12.011. Epub 2018 Jan 9. Biol Psychiatry Cogn Neurosci Neuroimaging. 2018. PMID: 29884282 Free PMC article. Review.
-
A mysterious sensation about sleep and health: the role of interoception.BMC Public Health. 2021 Aug 23;21(1):1584. doi: 10.1186/s12889-021-11603-0. BMC Public Health. 2021. PMID: 34425779 Free PMC article.
-
Mindfulness, Interoception, and Olfaction: A Network Approach.Brain Sci. 2020 Nov 29;10(12):921. doi: 10.3390/brainsci10120921. Brain Sci. 2020. PMID: 33260427 Free PMC article.
References
-
- Aarøe L, Petersen MB. Hunger games: Fluctuations in blood glucose levels influence support for social welfare. Psychological Science. 2013;24:2550–2556. - PubMed
-
- Aaronson ST, Carpenter LL, Conway CR, Reimherr FW, Lisanby SH, Schwartz TL, Bunker M. Vagus nerve stimulation therapy randomized to different amounts of electrical charge for treatment-resistant depression: Acute and chronic effects. Brain Stimulation. 2013;6:631–640. - PubMed
-
- Aarts H, Dijksterhuis A, Vries P. On the psychology of drinking: Being thirsty and perceptually ready. British Journal of Psychology. 2001;92:631–642. - PubMed
-
- Aarts H, Gollwitzer PM, Hassin RR. Goal contagion: Perceiving is for pursuing. Journal of Personality and Social Psychology. 2004;87:23–37. - PubMed
-
- Ádám G. Visceral perception: Understanding internal cognition. New York: Plenum Press; 1998.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
