

What really matters in end-of-life discussions? Perspectives of patients in hospital with serious illness and their families
- PMID: 25367427
- PMCID: PMC4259796
- DOI: 10.1503/cmaj.140673
What really matters in end-of-life discussions? Perspectives of patients in hospital with serious illness and their families
Abstract
Background: The guideline-recommended elements to include in discussions about goals of care with patients with serious illness are mostly based on expert opinion. We sought to identify which elements are most important to patients and their families.
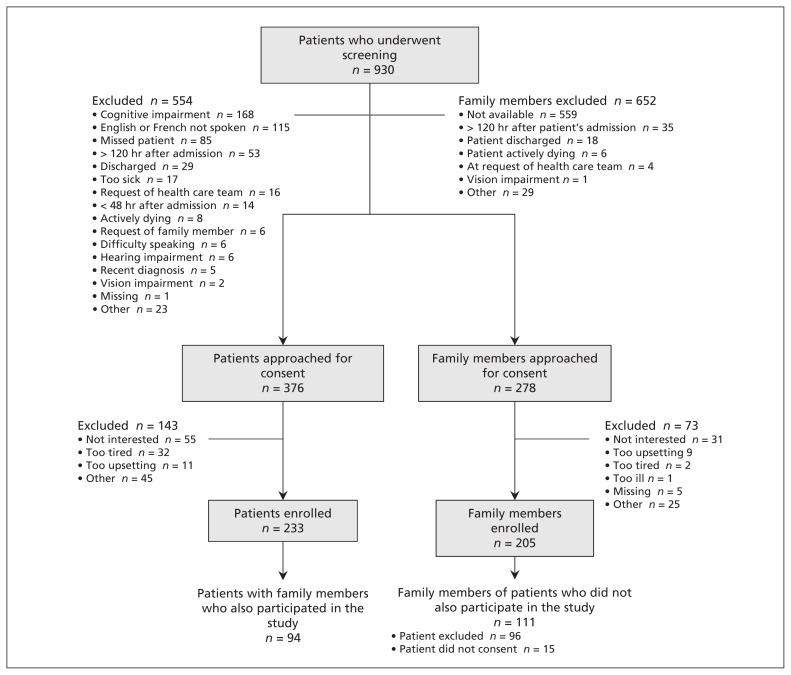
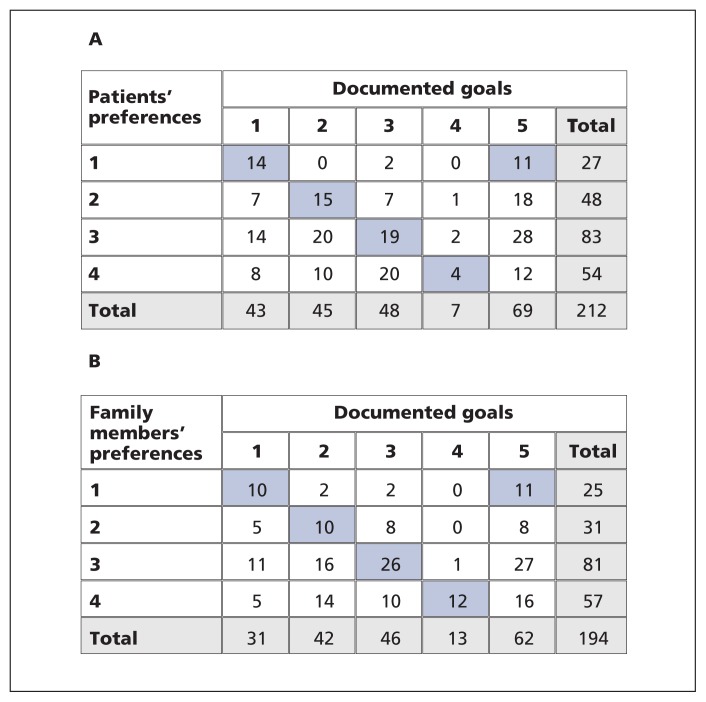
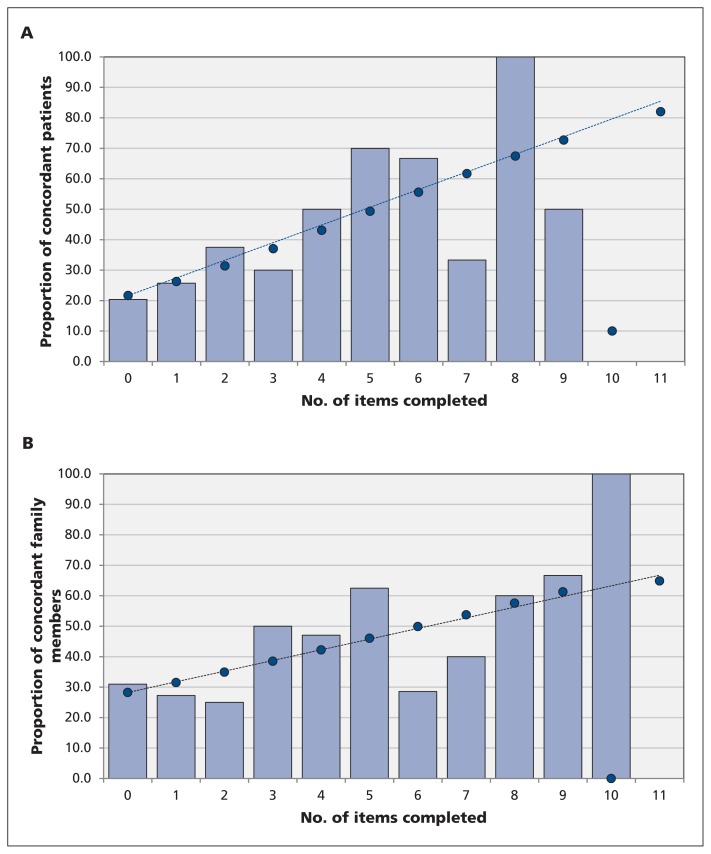
Methods: We used a cross-sectional study design involving patients from 9 Canadian hospitals. We asked older adult patients with serious illness and their family members about the occurrence and importance of 11 guideline-recommended elements of goals-of-care discussions. In addition, we assessed concordance between prescribed goals of care and patient preferences, and we measured patient satisfaction with goals-of-care discussions using the Canadian Health Care Evaluation Project (CANHELP) questionnaire.
Results: Our study participants included 233 patients (mean age 81.2 yr) and 205 family members (mean age 60.2 yr). Participants reported that clinical teams had addressed individual elements of goals-of-care discussions infrequently (range 1.4%-31.7%). Patients and family members identified the same 5 elements as being the most important to address: preferences for care in the event of life-threatening illness, values, prognosis, fears or concerns, and questions about goals of care. Addressing more elements was associated with both greater concordance between patients' preferences and prescribed goals of care, and greater patient satisfaction.
Interpretation: We identified elements of goals-of-care discussions that are most important to older adult patients in hospital with serious illness and their family members. We found that guideline-recommended elements of goals-of-care discussions are not often addressed by health care providers. Our results can inform interventions to improve the determination of goals of care in the hospital setting.
© 2014 Canadian Medical Association or its licensors.
Figures
Comment in
-
Goals of care are important for older adults with severe illness and their families, and are infrequently addressed by health professionals.Evid Based Nurs. 2015 Oct;18(4):126. doi: 10.1136/eb-2015-102078. Epub 2015 May 13. Evid Based Nurs. 2015. PMID: 25972591 No abstract available.
References
-
- Heyland DK, Lavery JV, Tranmer JE, et al. Dying in Canada: is it an institutionalized, technologically supported experience? J Palliat Care 2000;16(Suppl):S10–6. - PubMed
-
- Heyland DK, Lavery JV, Tranmer J, et al. The final days: an analysis of the dying experience in Ontario. Ann R Coll Physicians Surg Can 2000;33:356–61.
-
- Health Care Use at the End of Life in Western Canada. Ottawa: Canadian Institute for Health Information; 2007.
-
- Health Care Use at the End of Life in Atlantic Canada. Ottawa: Canadian Institute for Health Information; 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases