

Early Vertebroplasty versus Delayed Vertebroplasty for Acute Osteoporotic Compression Fracture : Are the Results of the Two Surgical Strategies the Same?
- PMID: 25368763
- PMCID: PMC4217057
- DOI: 10.3340/jkns.2014.56.3.211
Early Vertebroplasty versus Delayed Vertebroplasty for Acute Osteoporotic Compression Fracture : Are the Results of the Two Surgical Strategies the Same?
Abstract
Objective: In Korea, early vertebroplasty (EVP) or delayed vertebroplasty (DVP, which is performed at least 2 weeks after diagnosis) were performed for the treatment of acute osteoporotic compression fracture (OCF) of the spine. The present study compared the outcomes of two surgical strategies for the treatment of single-level acute OCF in the thoracolumbar junction (T12-L2).
Methods: From 2004 to 2010, 23 patients were allocated to the EVP group (EVPG) and 27 patients to the DVP group (DVPG). Overall mean age was 68.3±7.9 and minimum follow-up period was 1.0 year. Retrospective study of clinical and radiological results was conducted.
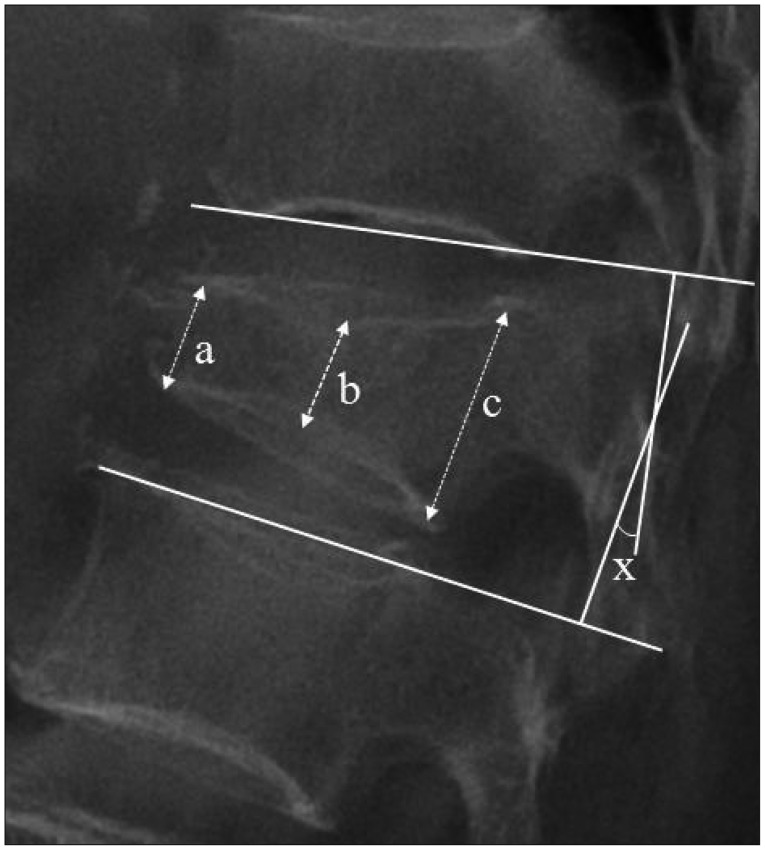
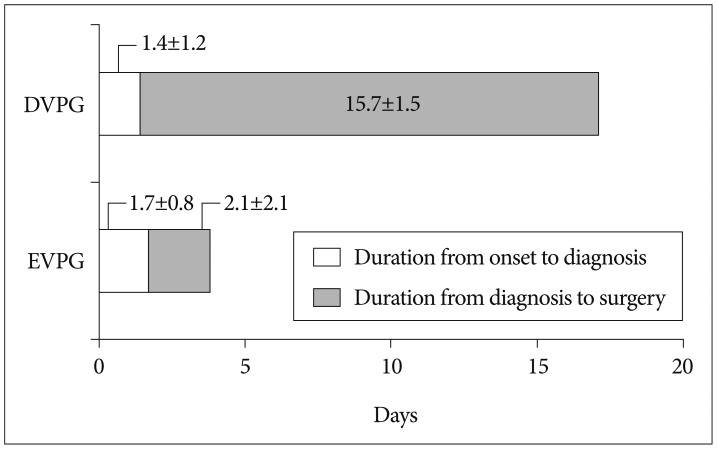
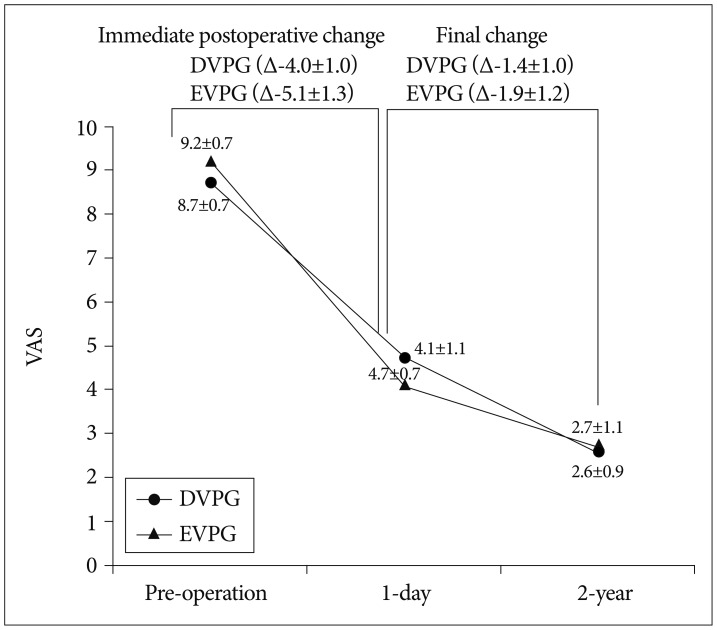
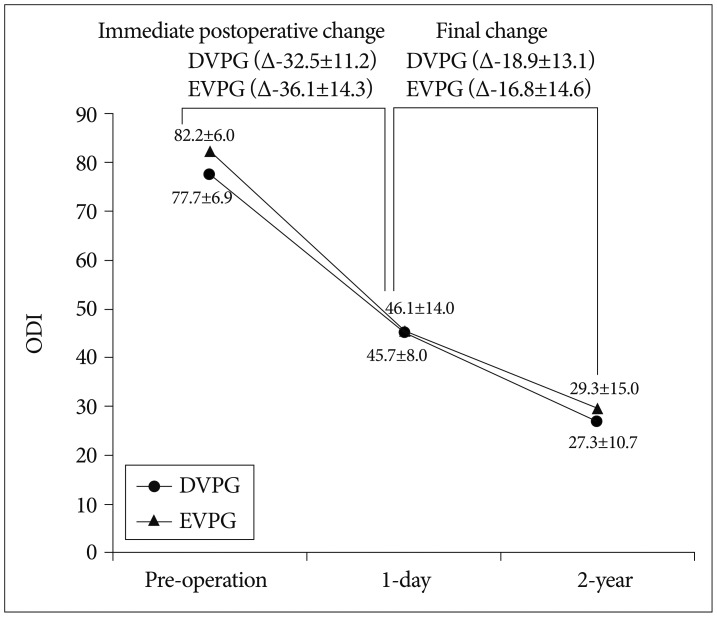
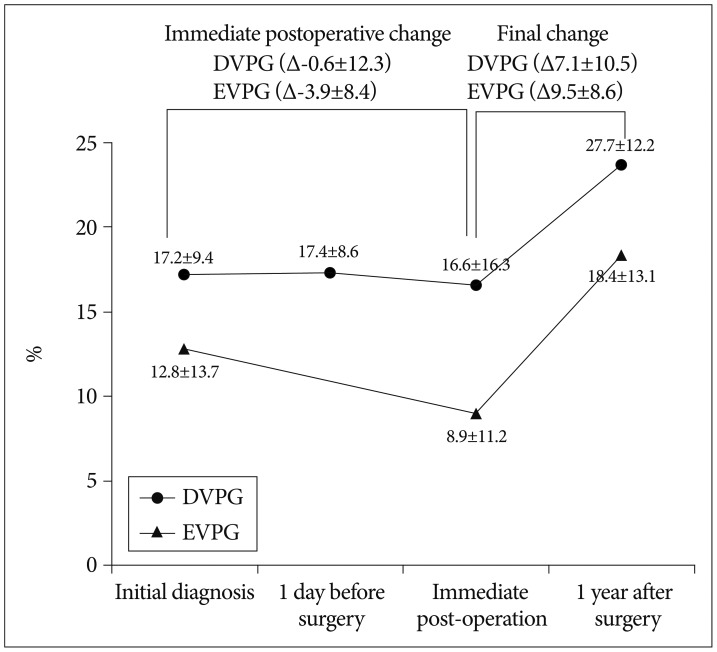
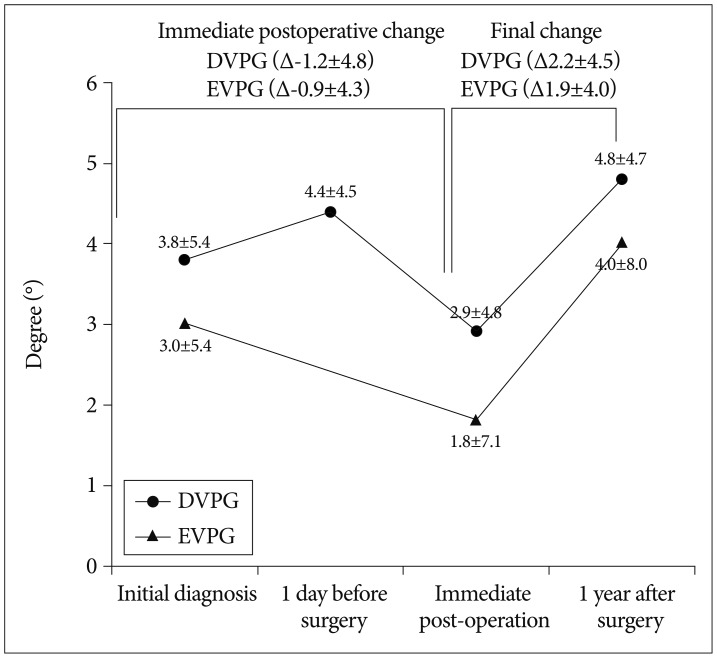
Results: No significant differences in baseline characteristics were observed between the two groups. As expected, mean duration from onset to vertebroplasty and mean duration of hospital stay were significantly longer in the DVPG (17.1±2.1 and 17.5±4.2) than in the EVPG (3.8±3.3 and 10.8±5.1, p=0.001). Final clinical outcome including visual analogue scale (VAS), Oswestry Disability Index, and Odom's criteria did not differ between the two groups. However, immediate improvement of the VAS after vertebroplasty was greater in the EVPG (5.1±1.3) than in the DVPG (4.0±1.0, p=0.002). The proportion of cement leakage was lower in the EVPG (30.4%) than in the DVPG (59.3%, p=0.039). In addition, semiquantitative grade of cement interdigitation was significantly more favorable in the EVPG than in the DVPG (p=0.003). Final vertebral body collapse and segmental kyphosis did not differ significantly between the two groups.
Conclusion: Our findings suggest that EVP achieves a better immediate surgical effect with more favorable cost-effectiveness.
Keywords: Compression fracture; Osteoporosis; Spine; Vertebroplasty.
Figures
References
-
- Alvarez L, Pérez-Higueras A, Granizo JJ, de Miguel I, Quiñones D, Rossi RE. Predictors of outcomes of percutaneous vertebroplasty for osteoporotic vertebral fractures. Spine (Phila Pa 1976) 2005;30:87–92. - PubMed
-
- Anselmetti GC, Corrao G, Monica PD, Tartaglia V, Manca A, Eminefendic H, et al. Pain relief following percutaneous vertebroplasty : results of a series of 283 consecutive patients treated in a single institution. Cardiovasc Intervent Radiol. 2007;30:441–447. - PubMed
-
- Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine (Phila Pa 1976) 2000;25:923–928. - PubMed
-
- Erkan S, Ozalp TR, Yercan HS, Okcu G. Does timing matter in performing kyphoplasty? Acute versus chronic compression fractures. Acta Orthop Belg. 2009;75:396–404. - PubMed
-
- Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993;8:1137–1148. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
