

Analysis of age and disease status as predictors of thyroid cancer-specific mortality using the Surveillance, Epidemiology, and End Results database
- PMID: 25369076
- PMCID: PMC4291211
- DOI: 10.1089/thy.2014.0116
Analysis of age and disease status as predictors of thyroid cancer-specific mortality using the Surveillance, Epidemiology, and End Results database
Abstract
Background: Age at diagnosis is incorporated into all relevant staging systems for differentiated thyroid carcinoma (DTC). There is growing evidence that a specific age cutoff may not be ideal for accurate risk stratification. We sought to evaluate the interplay between age and oncologic variables in patients with DTC using the largest cohort to date.
Methods: The Surveillance, Epidemiology, and End RESULTS (SEER) database was queried to identify patients with DTC as their only malignancy for the period 1973 to 2009. Multivariate analyses using a range of age cutoffs and age subgroupings were utilized in order to search for an optimal age that would provide the most significant risk stratification between young and old patients. The primary outcome was disease-specific survival (DSS) and covariates included: age, race, sex, tumor/nodal/metastasis (TNM) stage, decade of diagnosis, and radioactive iodine therapy.
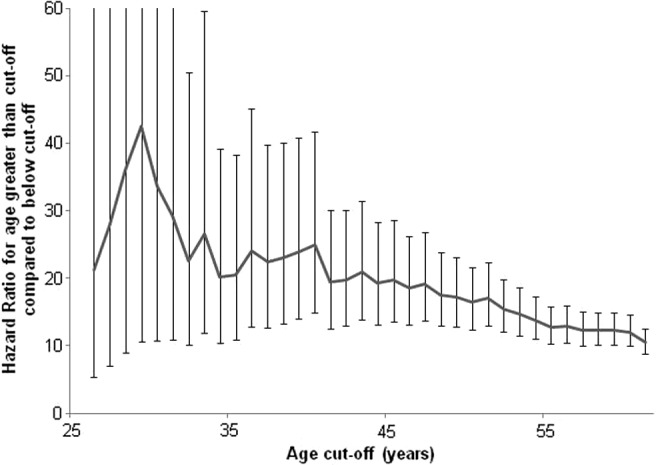
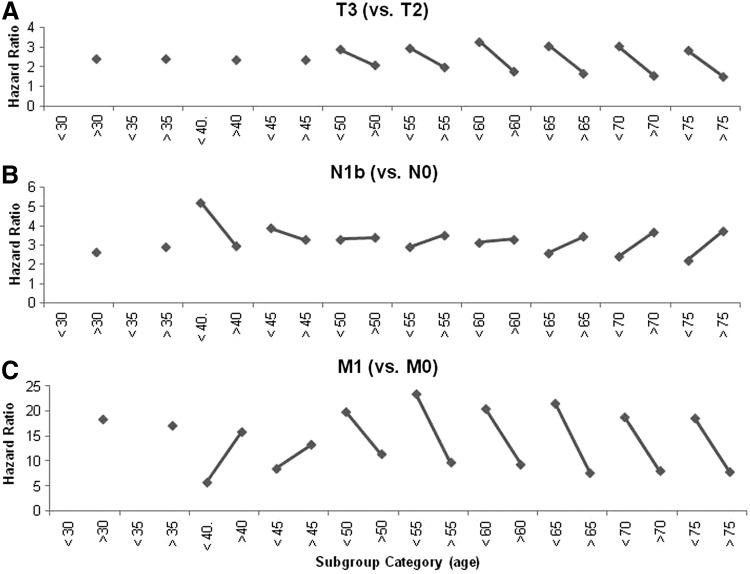
Results: A total of 85,740 patients were identified. Seventy-six percent of patients were American Joint Committee on Cancer (AJCC) stage I, 8% were stage II, 7% were stage III, and 8% were stage IV. Age over 45 years (hazard ratio [HR] 19.2, p<0.001) and metastatic disease (HR 13.1, p<0.001) were the strongest predictors of DSS. Other factors that significantly predicted DSS included: not receiving radioactive iodine (RAI; HR 1.3, p=0.002), T3 (HR 2.6, p<0.001), and T4 disease (HR 3.3, p<0.001), and nodal spread (HR 2.6 to 3.3, p<0.001). Female sex showed a significant protective effect (HR 0.7, p=0.001). Adjusting the age-group cutoff from 25 to 55 years showed consistently high HRs for advanced age, without a distinct change at any point. Comparing HRs for T, N, and M stage between young and old patient subgroups showed that advanced disease increased the risk for DSS regardless of age, and was oftentimes a worse prognosticator in young patient groups.
Conclusions: The contribution of age at diagnosis to a patient's DSS is considerable, but there is no age cutoff that affords any unique risk-stratification in patients with DTC.
Figures
Similar articles
-
Comparing the Prognostic Value of the Eighth Edition of the American Joint Committee on Cancer/Tumor Node Metastasis Staging System Between Papillary and Follicular Thyroid Cancer.Thyroid. 2018 Aug;28(8):976-981. doi: 10.1089/thy.2018.0066. Epub 2018 Jul 30. Thyroid. 2018. PMID: 29848239
-
Optimal Cutoff Age for Predicting Mortality Associated with Differentiated Thyroid Cancer.PLoS One. 2015 Jun 23;10(6):e0130848. doi: 10.1371/journal.pone.0130848. eCollection 2015. PLoS One. 2015. PMID: 26102084 Free PMC article.
-
Effect of Tumor Size on Risk of Metastatic Disease and Survival for Thyroid Cancer: Implications for Biopsy Guidelines.Thyroid. 2018 Mar;28(3):295-300. doi: 10.1089/thy.2017.0526. Epub 2018 Feb 22. Thyroid. 2018. PMID: 29373949
-
Surgical management of cervical lymph nodes in differentiated thyroid cancer.Otolaryngol Clin North Am. 2010 Apr;43(2):285-300, viii. doi: 10.1016/j.otc.2010.01.005. Otolaryngol Clin North Am. 2010. PMID: 20510715 Review.
-
Prognostic variables of papillary and follicular thyroid carcinoma patients with lymph node metastases and without distant metastases.Endocr Relat Cancer. 1999 Mar;6(1):109-15. doi: 10.1677/erc.0.0060109. Endocr Relat Cancer. 1999. PMID: 10732793 Review.
Cited by
-
HIF-1α and Caspase-3 expression in aggressive papillary thyroid carcinoma.World J Surg Oncol. 2022 Nov 4;20(1):353. doi: 10.1186/s12957-022-02815-8. World J Surg Oncol. 2022. PMID: 36329448 Free PMC article.
-
Risk of recurrence in patients with papillary thyroid carcinoma and minimal extrathyroidal extension not treated with radioiodine.J Endocrinol Invest. 2019 Jun;42(6):687-692. doi: 10.1007/s40618-018-0969-y. Epub 2018 Oct 23. J Endocrinol Invest. 2019. PMID: 30353424
-
Detection and Identification of Serum Peptides Biomarker in Papillary Thyroid Cancer.Med Sci Monit. 2018 Mar 17;24:1581-1587. doi: 10.12659/msm.907768. Med Sci Monit. 2018. PMID: 29549708 Free PMC article.
-
A Three-Domain Scoring System to Customize the Risk of Relapse of Differentiated Thyroid Carcinoma.Cancers (Basel). 2021 Aug 27;13(17):4335. doi: 10.3390/cancers13174335. Cancers (Basel). 2021. PMID: 34503146 Free PMC article.
-
Dynamic prediction of the risk of recurrence in patients over 60 years of age with differentiated thyroid carcinoma.Arch Endocrinol Metab. 2016 Aug;60(4):348-54. doi: 10.1590/2359-3997000000146. Epub 2016 Feb 23. Arch Endocrinol Metab. 2016. PMID: 26910621 Free PMC article.
References
-
- Siegel R, Ward E, Brawley O, Jemal A.2011Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 61:212–236 - PubMed
-
- Davies L, Welch HG.2006Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA 295:2164–2167 - PubMed
-
- Eustatia-Rutten CF, Corssmit EP, Biermasz NR, Pereira AM, Romijn JA, Smit JW.2006Survival and death causes in differentiated thyroid carcinoma. J Clin Endocrinol Metab 91:313–319 - PubMed
-
- Wong RM, Bresee C, Braunstein GD.2013Comparison with published systems of a new staging system for papillary and follicular thyroid carcinoma. Thyroid 23:566–574 - PubMed
-
- Byar DP, Green SB, Dor P, Williams ED, Colon J, van Gilse HA, Mayer M, Sylvester RJ, van Glabbeke M.1979. A prognostic index for thyroid carcinoma. A study of the E.O.R.T.C. Thyroid Cancer Cooperative Group. Eur J Cancer 15:1033–1041 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
