

Nonobstructive coronary artery disease and risk of myocardial infarction
- PMID: 25369489
- PMCID: PMC4893304
- DOI: 10.1001/jama.2014.14681
Nonobstructive coronary artery disease and risk of myocardial infarction
Abstract
Importance: Little is known about cardiac adverse events among patients with nonobstructive coronary artery disease (CAD).
Objective: To compare myocardial infarction (MI) and mortality rates between patients with nonobstructive CAD, obstructive CAD, and no apparent CAD in a national cohort.
Design, setting, and participants: Retrospective cohort study of all US veterans undergoing elective coronary angiography for CAD between October 2007 and September 2012 in the Veterans Affairs health care system. Patients with prior CAD events were excluded.
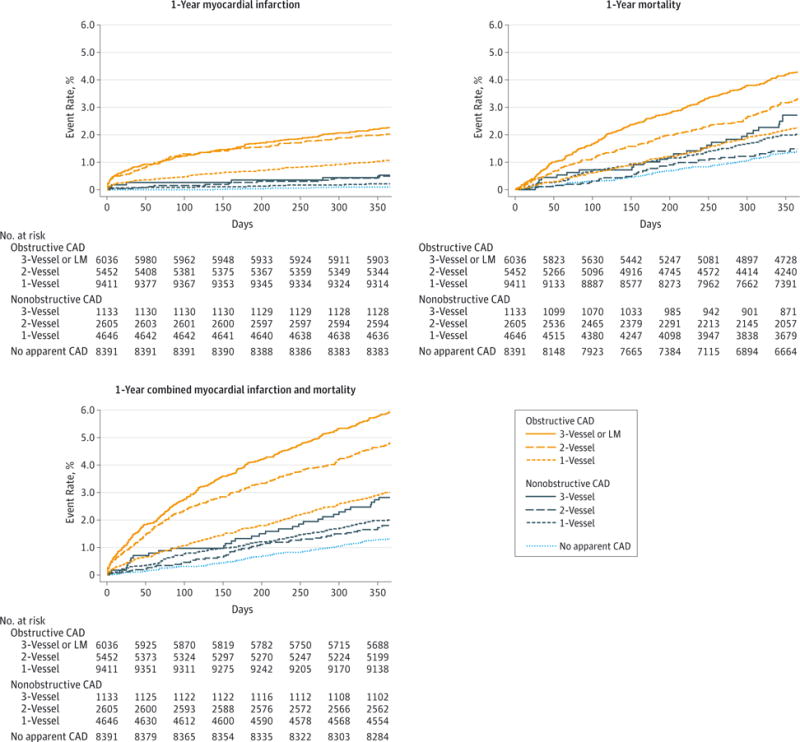
Exposures: Angiographic CAD extent, defined by degree (no apparent CAD: no stenosis >20%; nonobstructive CAD: ≥1 stenosis ≥20% but no stenosis ≥70%; obstructive CAD: any stenosis ≥70% or left main [LM] stenosis ≥50%) and distribution (1, 2, or 3 vessel).
Main outcomes and measures: The primary outcome was 1-year hospitalization for nonfatal MI after the index angiography. Secondary outcomes included 1-year all-cause mortality and combined 1-year MI and mortality.
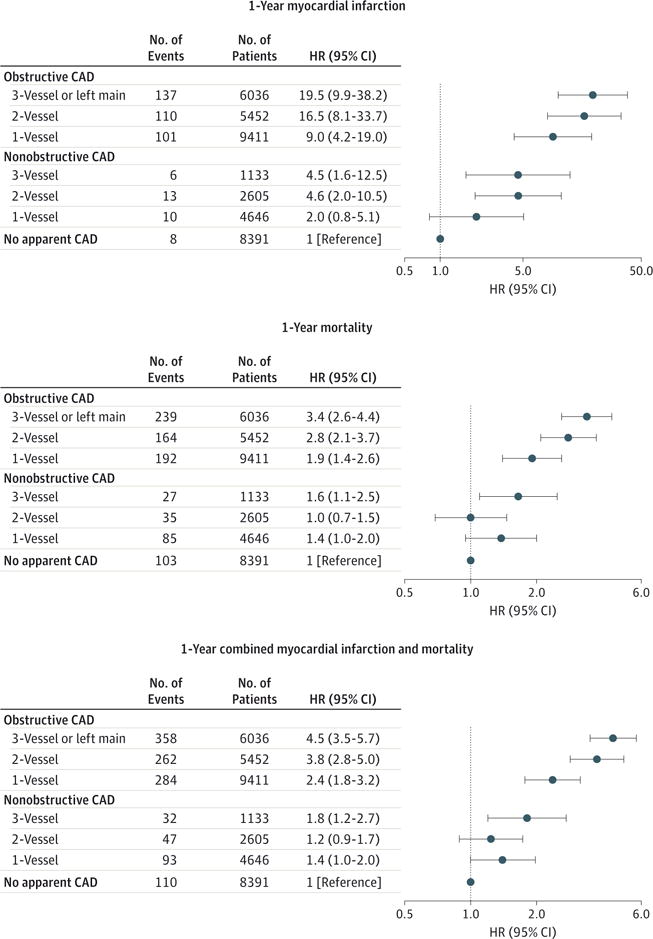
Results: Among 37,674 patients, 8384 patients (22.3%) had nonobstructive CAD and 20,899 patients (55.4%) had obstructive CAD. Within 1 year, 845 patients died and 385 were rehospitalized for MI. Among patients with no apparent CAD, the 1-year MI rate was 0.11% (n = 8, 95% CI, 0.10%-0.20%) and increased progressively by 1-vessel nonobstructive CAD, 0.24% (n = 10, 95% CI, 0.10%-0.40%); 2-vessel nonobstructive CAD, 0.56% (n = 13, 95% CI, 0.30%-1.00%); 3-vessel nonobstructive CAD, 0.59% (n = 6, 95% CI, 0.30%-1.30%); 1-vessel obstructive CAD, 1.18% (n = 101, 95% CI, 1.00%-1.40%); 2-vessel obstructive CAD, 2.18% (n = 110, 95% CI, 1.80%-2.60%); and 3-vessel or LM obstructive CAD, 2.47% (n = 137, 95% CI, 2.10%-2.90%). After adjustment, 1-year MI rates increased with increasing CAD extent. Relative to patients with no apparent CAD, patients with 1-vessel nonobstructive CAD had a hazard ratio (HR) for 1-year MI of 2.0 (95% CI, 0.8-5.1); 2-vessel nonobstructive HR, 4.6 (95% CI, 2.0-10.5); 3-vessel nonobstructive HR, 4.5 (95% CI, 1.6-12.5); 1-vessel obstructive HR, 9.0 (95% CI, 4.2-19.0); 2-vessel obstructive HR, 16.5 (95% CI, 8.1-33.7); and 3-vessel or LM obstructive HR, 19.5 (95% CI, 9.9-38.2). One-year mortality rates were associated with increasing CAD extent, ranging from 1.38% among patients without apparent CAD to 4.30% with 3-vessel or LM obstructive CAD. After risk adjustment, there was no significant association between 1- or 2-vessel nonobstructive CAD and mortality, but there were significant associations with mortality for 3-vessel nonobstructive CAD (HR, 1.6; 95% CI, 1.1-2.5), 1-vessel obstructive CAD (HR, 1.9; 95% CI, 1.4-2.6), 2-vessel obstructive CAD (HR, 2.8; 95% CI, 2.1-3.7), and 3-vessel or LM obstructive CAD (HR, 3.4; 95% CI, 2.6-4.4). Similar associations were noted with the combined outcome.
Conclusions and relevance: In this cohort of patients undergoing elective coronary angiography, nonobstructive CAD, compared with no apparent CAD, was associated with a significantly greater 1-year risk of MI and all-cause mortality. These findings suggest clinical importance of nonobstructive CAD and warrant further investigation of interventions to improve outcomes among these patients.
Conflict of interest statement
Figures
References
-
- Bugiardini R, Bairey Merz CN. Angina with “normal” coronary arteries: a changing philosophy. JAMA. 2005;293(4):477–484. - PubMed
-
- Patel MR, Chen AY, Peterson ED, et al. Prevalence, predictors, and outcomes of patients with non-ST-segment elevation myocardial infarction and insignificant coronary artery disease: results from the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines (CRUSADE) initiative. Am Heart J. 2006;152(4):641–647. - PubMed
-
- Roe MT, Harrington RA, Prosper DM, et al. Clinical and therapeutic profile of patients presenting with acute coronary syndromes who do not have significant coronary artery disease: the Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy (PURSUIT) Trial Investigators. Circulation. 2000;102(10):1101–1106. - PubMed
-
- Hung M-J, Cherng W-J. Comparison of white blood cell counts in acute myocardial infarction patients with significant versus insignificant coronary artery disease. Am J Cardiol. 2003;91(11):1339–1342. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
