

Cardiac MR assessment of cardiac myxomas
- PMID: 25369530
- PMCID: PMC4277385
- DOI: 10.1259/bjr.20140599
Cardiac MR assessment of cardiac myxomas
Abstract
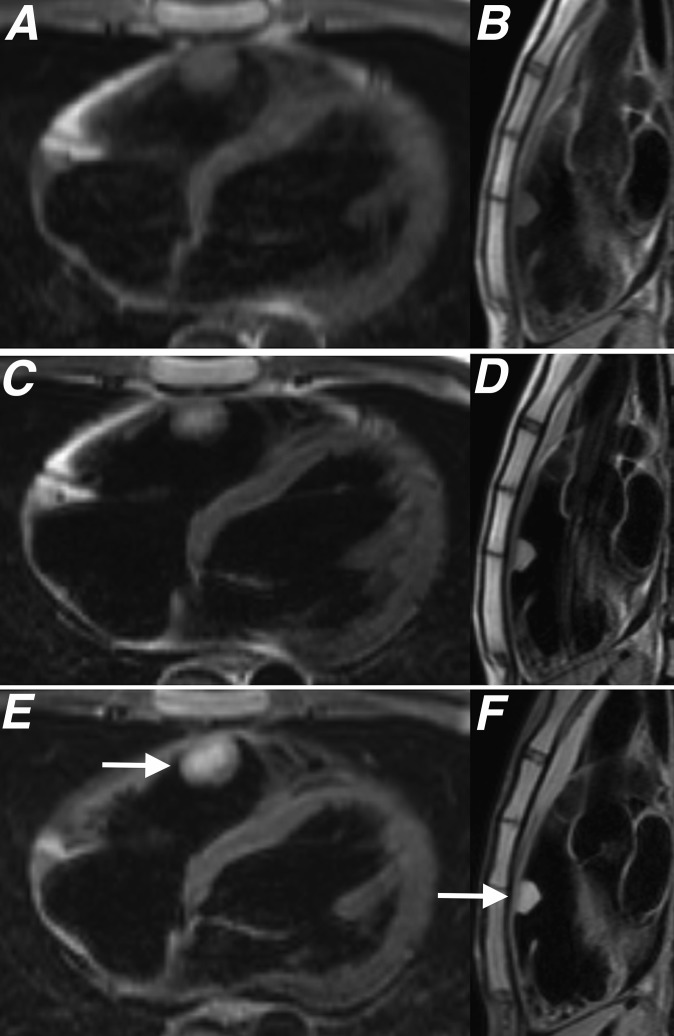
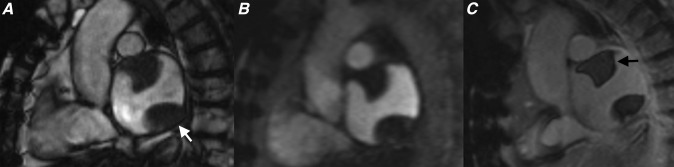
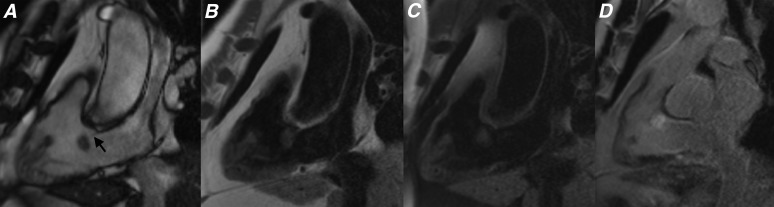
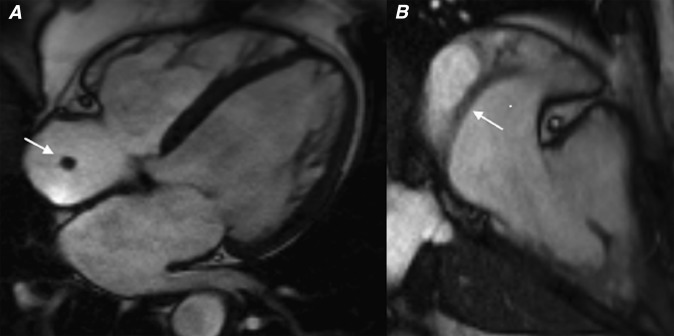
Cardiac myxomas are the most common benign primary cardiac tumour to present in adulthood. While most patients present with symptoms of cardiac obstruction, embolic phenomena or constitutional impairment, up to a fifth of patients remain asymptomatic and are incidentally diagnosed on imaging. Although echocardiography is usually the initial imaging modality used to evaluate these patients, cardiac MRI (CMR) has emerged over the past decade as the primary imaging modality in the assessment of patients with cardiac tumours. The superior tissue characterization capability of CMR means that it is able to determine the nature of some tumours pre-operatively and performs well in differentiating myxomas from thrombus. We present a pictorial review highlighting the key CMR features of myxomas and show how these lesions can be differentiated from thrombus and other cardiac masses.
Figures
References
-
- Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med 1993; 117: 1027–31. - PubMed
-
- Grebenc ML, Rosado-de-Christenson ML, Green CE, Burke AP, Galvin JR. Cardiac myxoma: imaging features in 83 patients. Radiographics 2002; 22: 673–89. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
