

First-in-human phase I study of pictilisib (GDC-0941), a potent pan-class I phosphatidylinositol-3-kinase (PI3K) inhibitor, in patients with advanced solid tumors
- PMID: 25370471
- PMCID: PMC4287394
- DOI: 10.1158/1078-0432.CCR-14-0947
First-in-human phase I study of pictilisib (GDC-0941), a potent pan-class I phosphatidylinositol-3-kinase (PI3K) inhibitor, in patients with advanced solid tumors
Abstract
Purpose: This first-in-human dose-escalation trial evaluated the safety, tolerability, maximal-tolerated dose (MTD), dose-limiting toxicities (DLT), pharmacokinetics, pharmacodynamics, and preliminary clinical activity of pictilisib (GDC-0941), an oral, potent, and selective inhibitor of the class I phosphatidylinositol-3-kinases (PI3K).
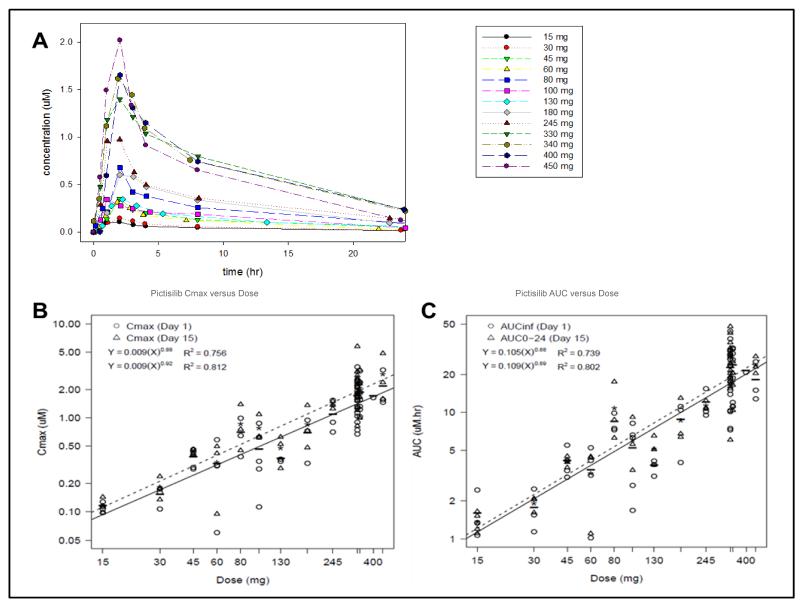
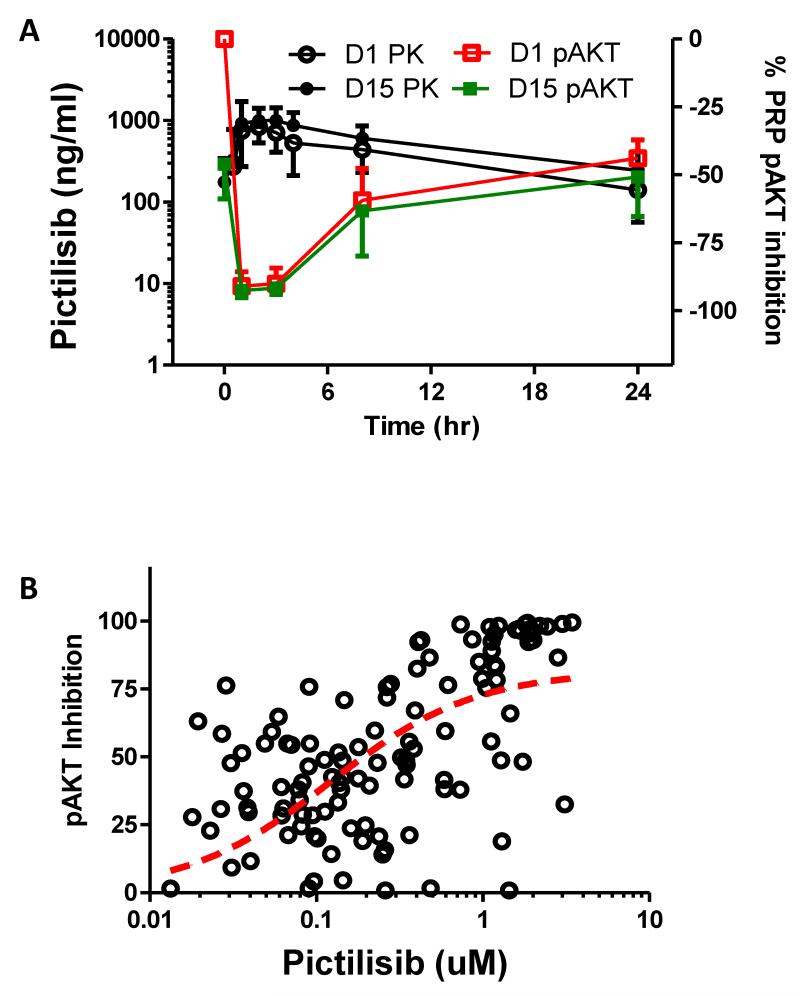
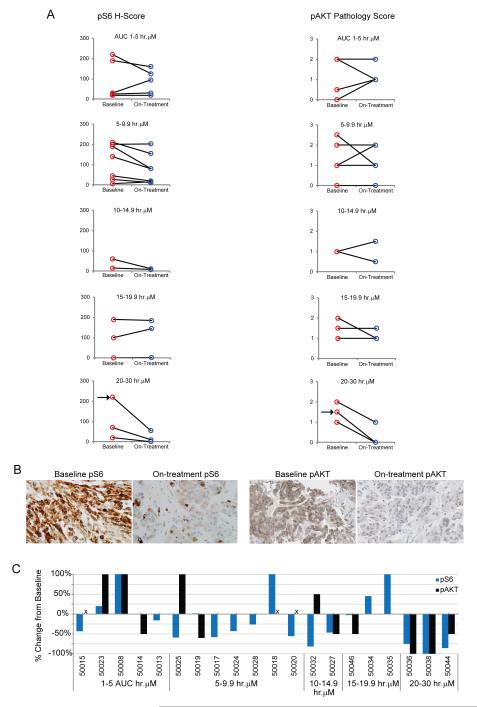
Patients and methods: Sixty patients with solid tumors received pictilisib at 14 dose levels from 15 to 450 mg once-daily, initially on days 1 to 21 every 28 days and later, using continuous dosing for selected dose levels. Pharmacodynamic studies incorporated (18)F-FDG-PET, and assessment of phosphorylated AKT and S6 ribosomal protein in platelet-rich plasma (PRP) and tumor tissue.
Results: Pictilisib was well tolerated. The most common toxicities were grade 1-2 nausea, rash, and fatigue, whereas the DLT was grade 3 maculopapular rash (450 mg, 2 of 3 patients; 330 mg, 1 of 7 patients). The pharmacokinetic profile was dose-proportional and supported once-daily dosing. Levels of phosphorylated serine-473 AKT were suppressed >90% in PRP at 3 hours after dose at the MTD and in tumor at pictilisib doses associated with AUC >20 h·μmol/L. Significant increase in plasma insulin and glucose levels, and >25% decrease in (18)F-FDG uptake by PET in 7 of 32 evaluable patients confirmed target modulation. A patient with V600E BRAF-mutant melanoma and another with platinum-refractory epithelial ovarian cancer exhibiting PTEN loss and PIK3CA amplification demonstrated partial response by RECIST and GCIG-CA125 criteria, respectively.
Conclusion: Pictilisib was safely administered with a dose-proportional pharmacokinetic profile, on-target pharmacodynamic activity at dose levels ≥100 mg and signs of antitumor activity. The recommended phase II dose was continuous dosing at 330 mg once-daily.
©2014 American Association for Cancer Research.
Figures
References
-
- Vanhaesebroeck B, Guillermet-Guibert J, Graupera M, Bilanges M. The emerging mechanisms of isoform-specific PI3K signalling. Nat Rev Mol Cell Biol. 2010;11:329–41. - PubMed
-
- Engelman JA. Targeting PI3K signalling in cancer: opportunities, challenges and limitations. Nat Rev Cancer. 2009;9:550–62. - PubMed
-
- Clarke PA, Workman P. Phosphatidylinositide-3-kinase inhibitors: addressing questions of isoform selectivity and pharmacodynamic/predictive biomarkers in early clinical trials. J Clin Oncol. 2012;30:331–3. - PubMed
-
- Sansal I, Sellers WR. The biology and clinical relevance of the PTEN tumor suppressor pathway. J Clin Oncol. 2004;22:2954–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
