

Baseline OCT measurements in the idiopathic intracranial hypertension treatment trial, part I: quality control, comparisons, and variability
- PMID: 25370510
- PMCID: PMC4266084
- DOI: 10.1167/iovs.14-14960
Baseline OCT measurements in the idiopathic intracranial hypertension treatment trial, part I: quality control, comparisons, and variability
Erratum in
-
Erratum.Invest Ophthalmol Vis Sci. 2016 Dec 1;57(15):6909. doi: 10.1167/iovs.14-14960a. Invest Ophthalmol Vis Sci. 2016. PMID: 28027563 Free PMC article. No abstract available.
Abstract
Purpose: Optical coherence tomography (OCT) has been used to investigate papilledema in single-site, mostly retrospective studies. We investigated whether spectral-domain OCT (SD-OCT), which provides thickness and volume measurements of the optic nerve head and retina, could reliably demonstrate structural changes due to papilledema in a prospective multisite clinical trial setting.
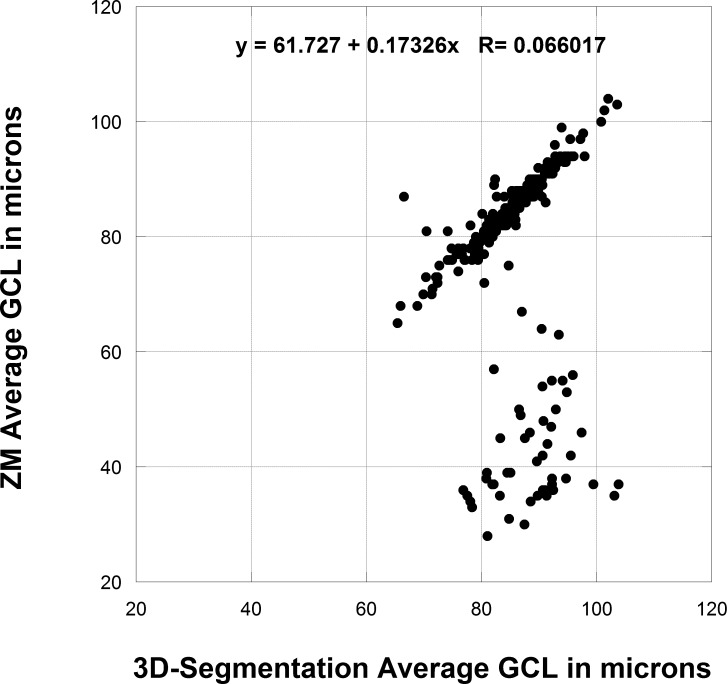
Methods: At entry, 126 subjects in the Idiopathic Intracranial Hypertension Treatment Trial (IIHTT) with mild visual field loss had optic disc and macular scans, using the Cirrus SD-OCT. Images were analyzed by using the proprietary commercial and custom 3D-segmentation algorithms to calculate retinal nerve fiber layer (RNFL), total retinal thickness (TRT), optic nerve head volume (ONHV), and retinal ganglion cell layer (GCL) thickness. We evaluated variability, with interocular comparison and correlation between results for both methods.
Results: The average RNFL thickness > 95% of normal controls in 90% of eyes and the RNFL, TRT, ONH height, and ONHV showed strong (r > 0.8) correlations for interocular comparisons. Variability for repeated testing of OCT parameters was low for both methods and intraclass correlations > 0.9 except for the proprietary GCL thickness. The proprietary algorithm-derived RNFL, TRT, and GCL thickness measurements had failure rates of 10%, 16%, and 20% for all eyes respectively, which were uncommon with 3D-segmentation-derived measurements. Only 7% of eyes had GCL thinning that was less than fifth percentile of normal age-matched control eyes by both methods.
Conclusions: Spectral-domain OCT provides reliable continuous variables and quantified assessment of structural alterations due to papilledema. (ClinicalTrials.gov number, NCT01003639.).
Keywords: OCT; intracranial hypertension; optical coherence tomography; papilledema.
Copyright 2014 The Association for Research in Vision and Ophthalmology, Inc.
Figures




References
-
- Corbett J, Savino P, Thompson H, et al. Visual loss in pseudotumor cerebri: follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol. 1982; 39: 461–474. - PubMed
-
- Wall M, George D. Idiopathic intracranial hypertension: a prospective study of 50 patients. Brain. 1991; 114: 155–180. - PubMed
-
- Garrett J, Corbett JJ, Braswell RA, Santiago M. The increasing incidence of IIH. The effect of obesity on frequency of occurrence in Mississippi. Ann Neurol. 2004; 56 (suppl 8): S69.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
