

Analysis of case series of milky urine: A single center and departmental clinical experience with emphasis on management perspectives: A prospective observational study
- PMID: 25371613
- PMCID: PMC4216542
- DOI: 10.4103/0974-7796.141002
Analysis of case series of milky urine: A single center and departmental clinical experience with emphasis on management perspectives: A prospective observational study
Abstract
Background: Milky urine can be due to chyluria or lipiduria due to nephrotic syndrome. Filarial chyluria usually responds to medical management while non-filarial cases may require surgical intervention.
Aim: To perform a prospective observational study in patients presenting with milky urine in our centre over a period of one year from July 2011 to June 2012, a complete biochemical work up and imaging to find out the site of leakage of lymph if it is a case of chyluria, its response to medical management and the requirement of surgical intervention.
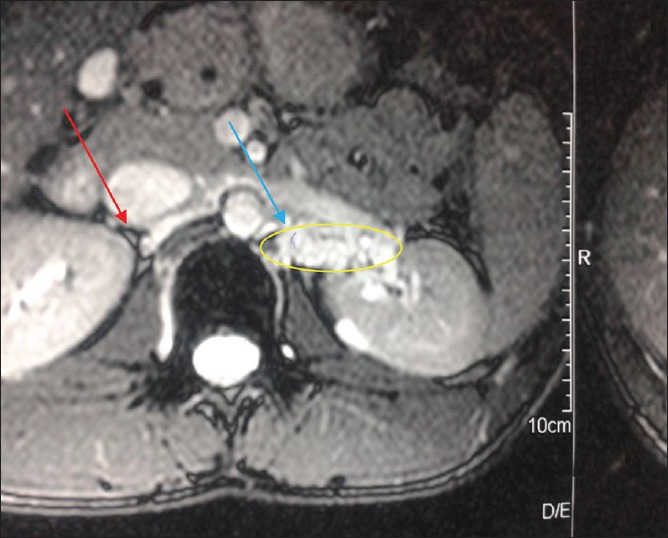
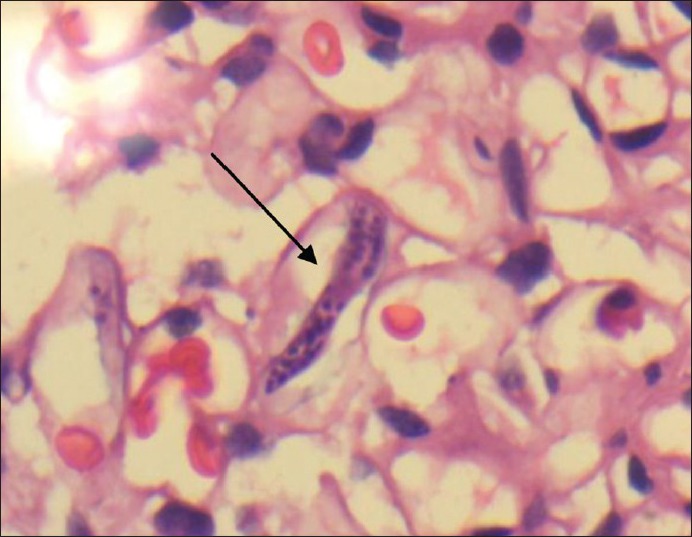
Materials and methods: Routine blood and urine investigations, 24 hour urine protein excretion, USG abdomen, serum lipid profile and rapid filarial antigen test were done in all. MRI abdomen was done in affordable patients. Renal biopsy was done in some chyluria patients for academic purpose and in milky urine with negative urine ether test. Sclerotherapy was done with 50% dextrose and 0.2% povidone iodine. Patients were followed up with 24 hour urine protein and triglyceride estimation.
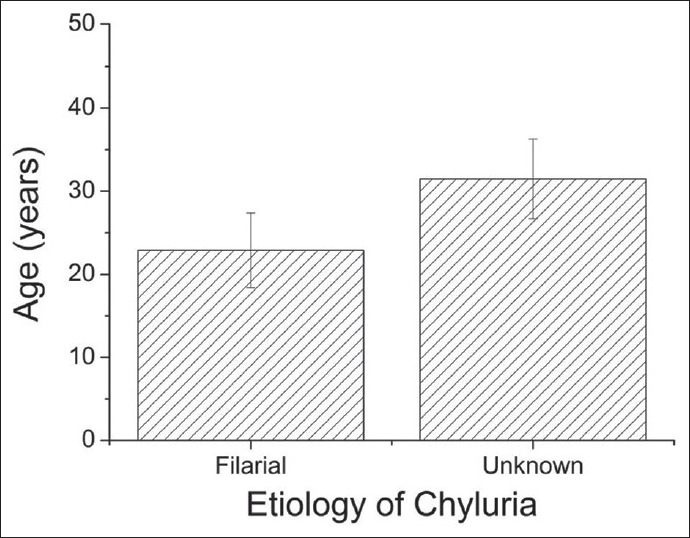
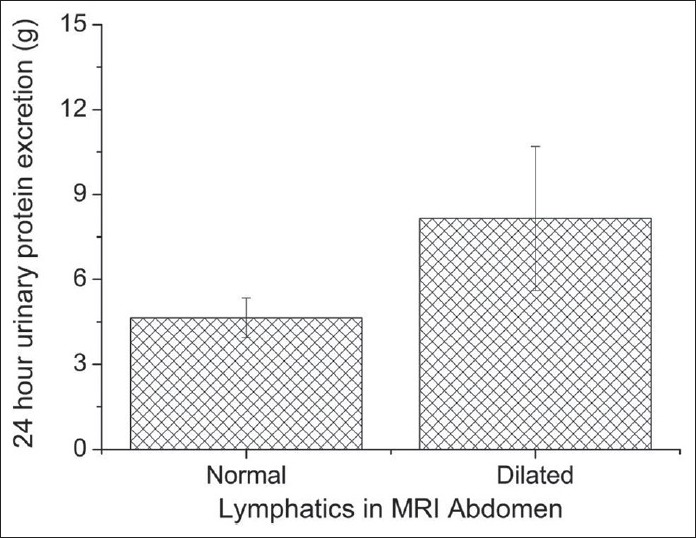
Results: 18 cases of milky urine were encountered. 8 were filarial chyluria, 9 non- filarial and 1 MCD. Mean urine TG level and median 24 hour urinary protein excretion were 37.2 ± 24.6 mg% and 4.96 g respectively. The mean age for filariasis (22.9 ± 4.5 years) was significantly different from that of non-filarial etiology (31.5 ± 4.8 years) (P = 0.005). The mean 24 hour urinary protein for normal MRI cases (4.64 ± 0.70 g) was significantly different from those with dilated lymphatics (8.15 ± 2.55 g) (P = 0.02). All the non- filarial and 4 filarial cases required sclerotherapy. One patient required a second sitting.
Conclusion: Milky urine is most commonly due to chyluria and occasionally due to nephrotic syndrome. Nephrotic syndrome is managed in its own way while chyluria not amenable to pharmacological intervention is managed with sclerotherapy.
Keywords: Chyluria; milky urine; sclerotherapy.
Conflict of interest statement
Figures

References
-
- Cheng JT, Mohan S, Nasr SH, D’Agati VD. Chyluria presenting as milky urine and nephrotic-range proteinuria. Kidney Int. 2006;70:1518–22. - PubMed
-
- Sharma S, Hemal AK. Chyluria-an overview. Int J Nephrol Urol. 2009;1:14–26.
-
- Lazarus JA, Marks MS. Non-parasitic chyluria with special reference to traumatic chyluria. J Urol. 1946;56:246–58. - PubMed
-
- Akisada M, Tani S. Filarial chyluria in Japan-lymphography, etiology and treatment in 30 cases. Radiology. 1968;90:311–7.
-
- Tandon V, Singh H, Dwivedi US, Mahmood M, Singh PB. Filarial chyluria: Long-term experience of a university hospital in India. Int J Urol. 2004;11:193–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
