

Comparison of clinical manifestations and outcomes between hepatitis B virus- and hepatitis C virus-related hepatocellular carcinoma: analysis of a nationwide cohort
- PMID: 25372403
- PMCID: PMC4221592
- DOI: 10.1371/journal.pone.0112184
Comparison of clinical manifestations and outcomes between hepatitis B virus- and hepatitis C virus-related hepatocellular carcinoma: analysis of a nationwide cohort
Erratum in
-
Correction: Comparison of Clinical Manifestations and Outcomes between Hepatitis B Virus- and Hepatitis C Virus-Related Hepatocellular Carcinoma: Analysis of a Nationwide Cohort.PLoS One. 2015 Jan 23;10(1):e0116652. doi: 10.1371/journal.pone.0116652. eCollection 2015. PLoS One. 2015. PMID: 25615935 Free PMC article.
Abstract
Background: We analyzed whether difference exist in the clinical manifestations and outcomes of hepatocellular carcinoma (HCC) according to the two major etiologies of HCC from a nationwide, population-based, random HCC registry.
Methods: Of the 31,521 new HCC cases registered at the Korea Central Cancer Registry between 2003 and 2005, 4,630 (14.7%) were randomly abstracted, and followed up until December 2011. Of those, 2,785 hepatitis B virus (HBV)-related and 447 hepatitis C virus (HCV)-related HCC patients were compared.
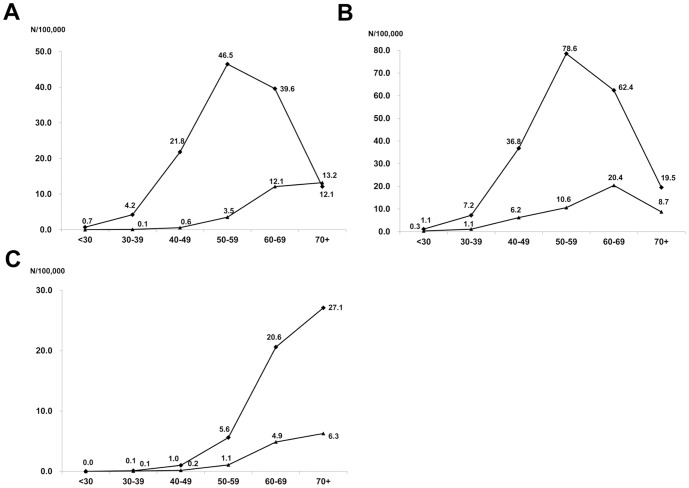
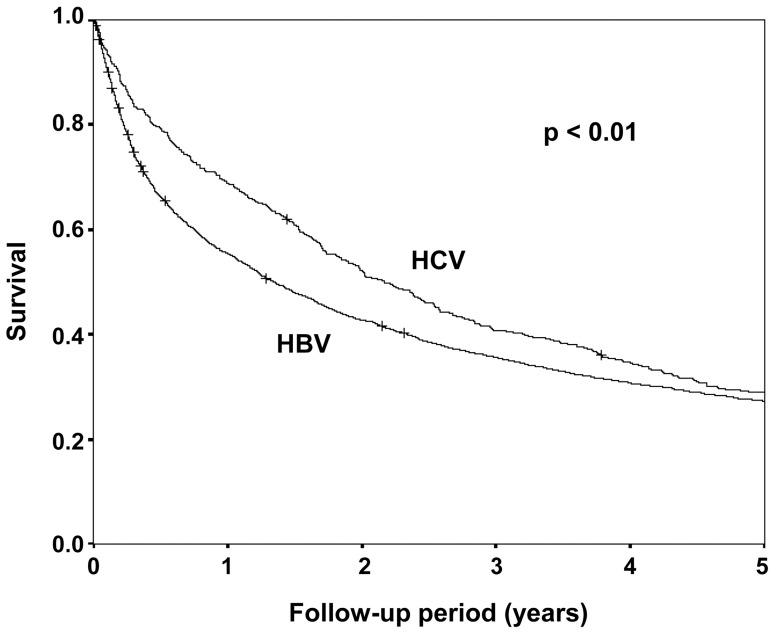
Results: The mean annual incidence rates of HBV- and HCV-related HCC incidence per 100,000 persons were 20.8 and 4.9, respectively. The annual incidence rate of HBV-related HCC peaked at 50-59 age group (46.5 per 100,000 persons), while the annual incidence rate of HCV-related HCC increased gradually to the ≥ 70 year age group (13.2 per 100,000 persons). Large tumors (≥ 5 cm) and portal vein invasion at initial diagnosis were more frequent in HBV-related HCC, while multiple tumors were more frequent in HCV-related HCC. In outcome analysis, HBV-related HCC showed poorer survival than HCV-related HCC [median survival: 1.34 vs. 2.17 years, adjusted hazard ratio (95% confidence interval): 0.88 (0.78-0.98), P = 0.03, adjusted for age, gender, Child-Pugh class, AJCC/mUICC stage, and initial treatment modality]. However, when divided according to the AJCC/mUICC stage, survival difference was observed only for those with AJCC/mUICC stage IV tumor, but not for AJCC/mUICC stage I, II or III tumors. The treatment outcome of each modality (resection, ablation, and transartherial chemoeombolization) was comparable between the two etiologies.
Conclusion: HBV-related and HCV-related HCC have clear differences in clinical manifestation, requiring different screening strategy according to etiology to optimize HCC surveillance in HBV-endemic area. However, etiology did not affect treatment outcomes and long-term survival within the same stage except for far advanced tumors.
Conflict of interest statement
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, et al. (2014) Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 13 doi: []10.1022/ijc.29210. [Epub ahead of print] - DOI - PubMed
-
- El-Serag HB (2011) Hepatocellular carcinoma. N Engl J Med 365: 1118–1127. - PubMed
-
- Forner A, Llovet JM, Bruix J (2012) Hepatocellular carcinoma. Lancet 379: 1245–1255. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
