

Weight loss in nonalcoholic Fatty liver disease patients in an ambulatory care setting is largely unsuccessful but correlates with frequency of clinic visits
- PMID: 25375228
- PMCID: PMC4222918
- DOI: 10.1371/journal.pone.0111808
Weight loss in nonalcoholic Fatty liver disease patients in an ambulatory care setting is largely unsuccessful but correlates with frequency of clinic visits
Abstract
Background and aims: Nonalcoholic fatty liver disease (NALFD) is a leading cause of liver disease. Weight loss improves clinical features of NAFLD; however, maintenance of weight loss outside of investigational protocols is poor. The goals of this study were to characterize patterns and clinical predictors of long-term weight loss in ambulatory patients with NAFLD.
Methods: We retrospectively reviewed 924 non-cirrhotic patients with NAFLD presenting to a liver clinic from May 1st 2007 to April 30th 2013. Overweight and obese patients were counseled on lifestyle modifications for weight loss as per USPSTF guidelines. The primary outcome was percent weight change between the first and last recorded visits: % weight change = (weightinitial - weightfinal)/(weightinitial). Baseline BMI and percent BMI change were secondary measures. Predictors of weight loss were determined using logistic regression.
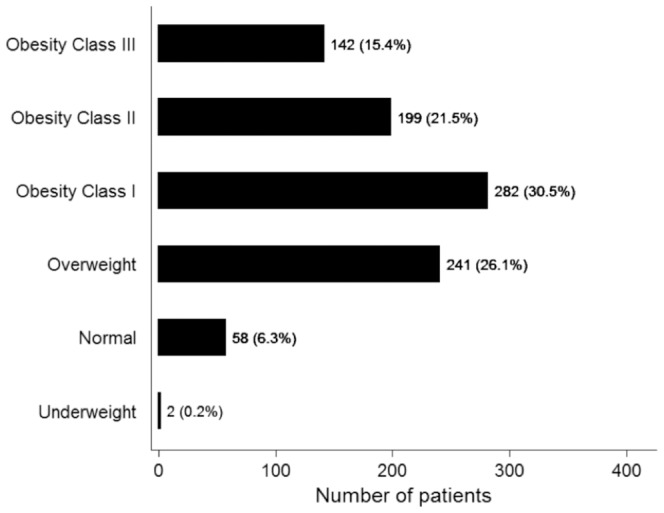
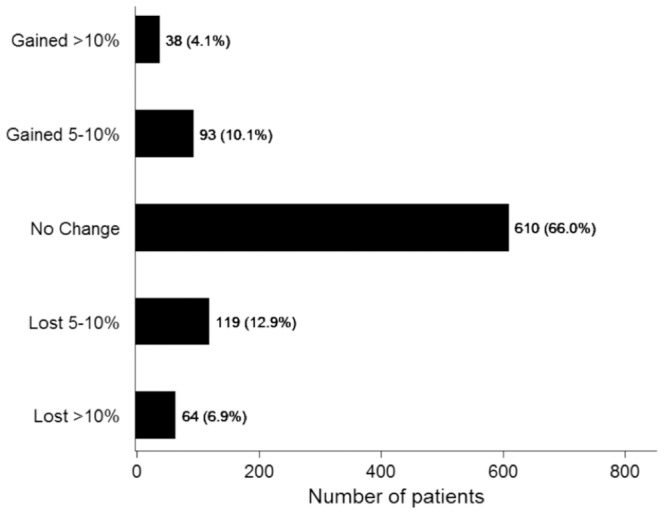
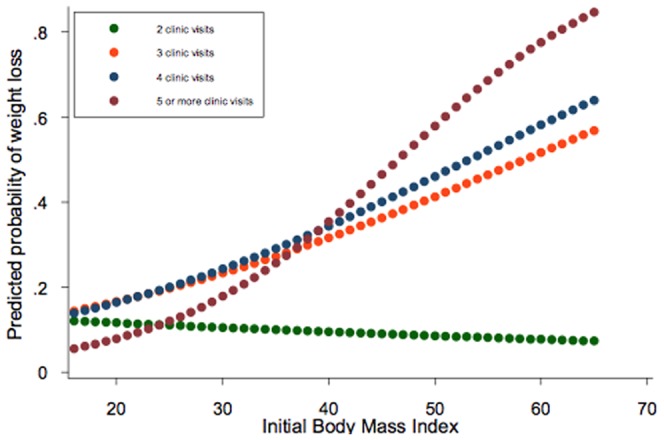
Results: The mean baseline BMI was 33.3±6.6 kg/m2, and the mean follow-up duration was 17.3±17.6 months. Most patients with NAFLD were in either overweight (26.1%) or class I obesity (30.5%) categories at baseline, while the prevalence of underweight and class III obesity was lower (0.2% and 15.4%, respectively). Overall, there was no change in mean weight or BMI during the follow-up period, and only 183 patients (19.8%) lost at least 5% body weight during the follow up period. Independent predictors of weight loss included number of clinic visits and baseline BMI, and patients with higher baseline BMI required more clinic visits to lose weight.
Conclusions: Weight loss is largely unsuccessful in NAFLD patients in the ambulatory care setting. Frequent clinical encounters are associated with weight reduction, especially among individuals with high baseline BMI. Future studies are required to define effective weight loss strategies in NAFLD patients.
Conflict of interest statement
Figures
References
-
- Targher G, Day CP, Bonora E (2010) Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med 363: 1341–1350. - PubMed
-
- Vernon G, Baranova A, Younossi ZM (2011) Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 34: 274–285. - PubMed
-
- Williams CD, Stengel J, Asike MI, Torres DM, Shaw J, et al. (2011) Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 140: 124–131. - PubMed
-
- Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, et al. (2004) Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology 40: 1387–1395. - PubMed
-
- Amarapurkar DN, Hashimoto E, Lesmana LA, Sollano JD, Chen PJ, et al. (2007) How common is non-alcoholic fatty liver disease in the Asia-Pacific region and are there local differences? J Gastroenterol Hepatol 22: 788–793. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
