

Trends in mechanical ventilation among patients hospitalized with acute exacerbations of COPD in the United States, 2001 to 2011
- PMID: 25375230
- PMCID: PMC4388126
- DOI: 10.1378/chest.14-1216
Trends in mechanical ventilation among patients hospitalized with acute exacerbations of COPD in the United States, 2001 to 2011
Abstract
Background: The use of noninvasive ventilation (NIV) in acute exacerbation of COPD has increased over time. However, little is known about patient factors influencing its use in routine clinical practice.
Methods: This was a retrospective cohort study of 723,560 hospitalizations for exacerbation of COPD at 475 hospitals between 2001 and 2011. The primary study outcome was the initial form of ventilation (NIV or invasive mechanical ventilation [IMV]). Hierarchical generalized linear models were used to examine the trends in ventilation and patient characteristics associated with receipt of NIV.
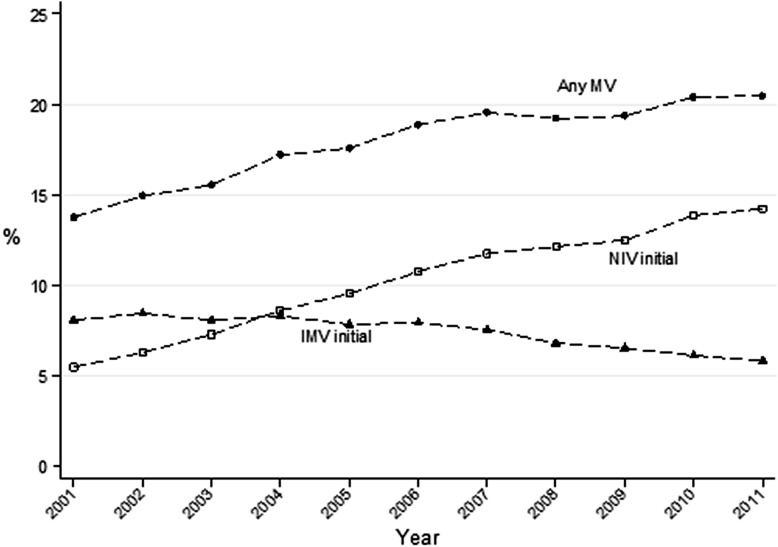
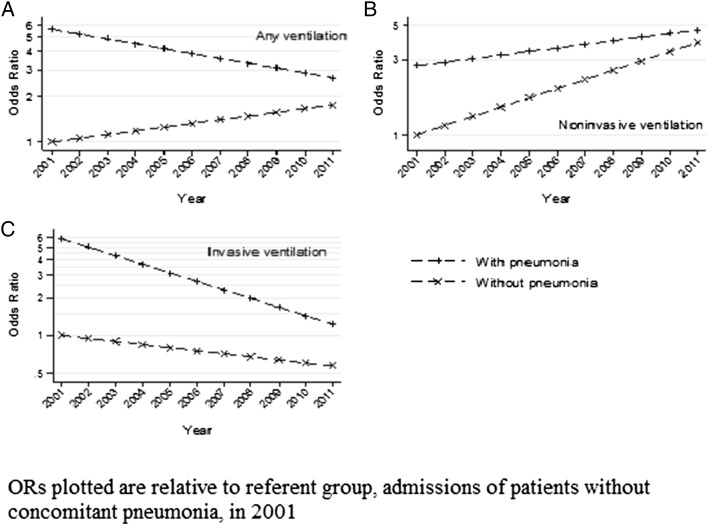
Results: After adjusting for patient and hospital characteristics, initial NIV increased by 15.1% yearly (from 5.9% to 14.8%), and initial IMV declined by 3.2% yearly (from 8.7% to 5.9%); annual exposure to any form of mechanical ventilation increased by 4.4% (from 14.1% to 20.3%). Among case subjects treated with ventilation, those aged ≥ 85 years had a 22% higher odds of receiving NIV compared with those aged < 65 years, while blacks (OR, 0.86) and Hispanics (OR, 0.91) were less likely to be treated with NIV than were whites. Cases with a high burden of comorbidities and those with concomitant pneumonia had high rates of NIV failure and were more likely to receive initial IMV. Use of NIV increased at a faster rate among the admissions of the oldest patients relative to the youngest.
Conclusions: The use of NIV for COPD exacerbations has increased steadily, whereas IMV use has declined. Several patient factors, including age, race, and comorbidities, influenced the receipt of NIV. Further research is needed to identify the factors driving these patterns.
Figures
Similar articles
-
Outcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary disease.JAMA Intern Med. 2014 Dec;174(12):1982-93. doi: 10.1001/jamainternmed.2014.5430. JAMA Intern Med. 2014. PMID: 25347545 Free PMC article.
-
Hospital patterns of mechanical ventilation for patients with exacerbations of COPD.Ann Am Thorac Soc. 2015 Mar;12(3):402-9. doi: 10.1513/AnnalsATS.201407-293OC. Ann Am Thorac Soc. 2015. PMID: 25654431 Free PMC article. Clinical Trial.
-
Outcomes of Noninvasive and Invasive Ventilation in Patients Hospitalized with Asthma Exacerbation.Ann Am Thorac Soc. 2016 Jul;13(7):1096-104. doi: 10.1513/AnnalsATS.201510-701OC. Ann Am Thorac Soc. 2016. PMID: 27070493 Free PMC article.
-
[Management of acute exacerbations of COPD].Rev Mal Respir. 2010 Oct;27(8):939-53. doi: 10.1016/j.rmr.2010.08.003. Rev Mal Respir. 2010. PMID: 20965408 Review. French.
-
Non-invasive ventilation in chronic obstructive pulmonary disease.J Physiol Pharmacol. 2004 Sep;55 Suppl 3:115-9. J Physiol Pharmacol. 2004. PMID: 15611602 Review.
Cited by
-
Resource use, characteristics and outcomes of prolonged non-invasive ventilation: a single-centre observational study in China.BMJ Open. 2018 Dec 4;8(12):e019271. doi: 10.1136/bmjopen-2017-019271. BMJ Open. 2018. PMID: 30518577 Free PMC article.
-
Intensive Care Unit Admission and Survival among Older Patients with Chronic Obstructive Pulmonary Disease, Heart Failure, or Myocardial Infarction.Ann Am Thorac Soc. 2017 Jun;14(6):943-951. doi: 10.1513/AnnalsATS.201611-847OC. Ann Am Thorac Soc. 2017. PMID: 28208030 Free PMC article.
-
Hospital Noninvasive Ventilation Case Volume and Outcomes of Acute Exacerbations of Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2016 Oct;13(10):1752-1759. doi: 10.1513/AnnalsATS.201603-209OC. Ann Am Thorac Soc. 2016. PMID: 27404021 Free PMC article.
-
A Cross-sectional Study of Hospital Performance on ICU Utilization Practices for Patients with Chronic Obstructive Pulmonary Disease.Lung. 2020 Aug;198(4):637-644. doi: 10.1007/s00408-020-00364-z. Epub 2020 Jun 3. Lung. 2020. PMID: 32495192 Free PMC article.
-
A Multicenter Retrospective Study Predicting Early Noninvasive Ventilation Failure in Patients With Acute Hypoxic Respiratory Failure.Clin Respir J. 2025 Jul;19(7):e70098. doi: 10.1111/crj.70098. Clin Respir J. 2025. PMID: 40588773 Free PMC article.
References
-
- FastStats. Chronic obstructive pulmonary disease (COPD) includes: chronic bronchitis and emphysema. CDC website. http://www.cdc.gov/nchs/fastats/copd.htm. Centers for Disease Control and Prevention website. Accessed December 10, 2013.
-
- NHLBI morbidity and mortality chartbook. National Heart, Lung, and Blood Institute website. https://www.nhlbi.nih.gov/files/docs/research/2012_ChartBook_508.pdf. Accessed March 11, 2014.
-
- Todisco T, Baglioni S, Eslami A, et al. Treatment of acute exacerbations of chronic respiratory failure: integrated use of negative pressure ventilation and noninvasive positive pressure ventilation. Chest. 2004;125(6):2217-2223. - PubMed
-
- Brochard L, Mancebo J, Wysocki M, et al. Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 1995;333(13):817-822. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
