

Hilar cholangiocarcinoma: controversies on the extent of surgical resection aiming at cure
- PMID: 25376337
- PMCID: PMC4304009
- DOI: 10.1007/s00384-014-2063-z
Hilar cholangiocarcinoma: controversies on the extent of surgical resection aiming at cure
Abstract
Background: Hilar cholangiocarcinoma is the most common malignant tumor affecting the extrahepatic bile duct. Surgical treatment offers the only possibility of cure, and it requires removal of all tumoral tissues with adequate resection margins. The aims of this review are to summarize the findings and to discuss the controversies on the extent of surgical resection aiming at cure for hilar cholangiocarcinoma.
Methods: The English medical literatures on hilar cholangiocarcinoma were studied to review on the relevance of adequate resection margins, routine caudate lobe resection, extent of liver resection, and combined vascular resection on perioperative and long-term survival outcomes of patients with resectable hilar cholangiocarcinoma.
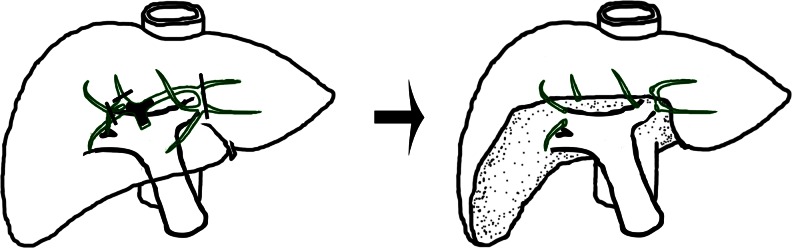
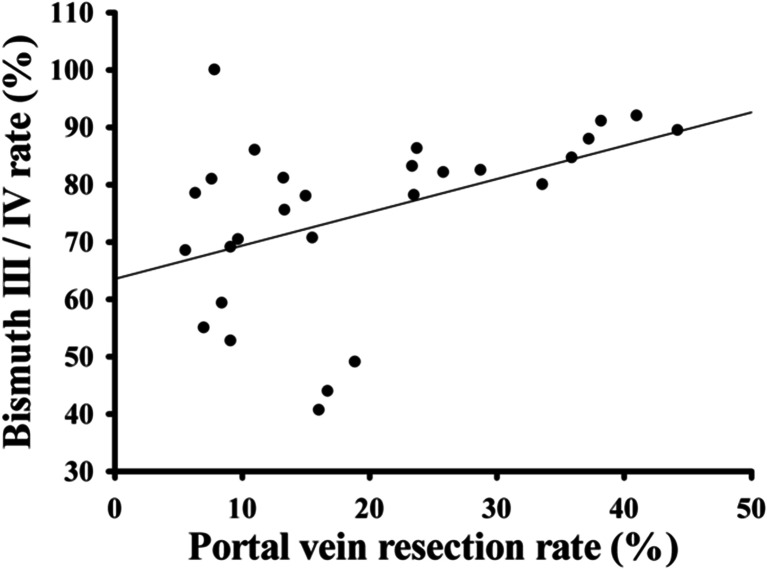
Results: Complete resection of tumor represents the most important prognostic factor of long-term survival for hilar cholangiocarcinoma. The primary aim of surgery is to achieve R0 resection. When R1 resection is shown intraoperatively, further resection is recommended. Combined hepatic resection is now generally accepted as a standard procedure even for Bismuth type I/II tumors. Routine caudate lobe resection is also advocated for cure. The extent of hepatic resection remains controversial. Most surgeons recommend major hepatic resection. However, minor hepatic resection has also been advocated in most patients. The decision to carry out right- or left-sided hepatectomy is made according to the predominant site of the lesion. Portal vein resection should be considered when its involvement by tumor is suspected.
Conclusion: The curative treatment of hilar cholangiocarcinoma remains challenging. Advances in hepatobiliary techniques have improved the perioperative and long-term survival outcomes of this tumor.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
