

AKI complications in critically ill patients: association with mortality rates and RRT
- PMID: 25376761
- PMCID: PMC4284413
- DOI: 10.2215/CJN.04750514
AKI complications in critically ill patients: association with mortality rates and RRT
Abstract
Background and objectives: AKI is associated with short- and long-term mortality. However, the exact contribution of AKI complications to the burden of mortality and whether RRT has any beneficial effect on reducing mortality rates in critically ill AKI patients are unknown.
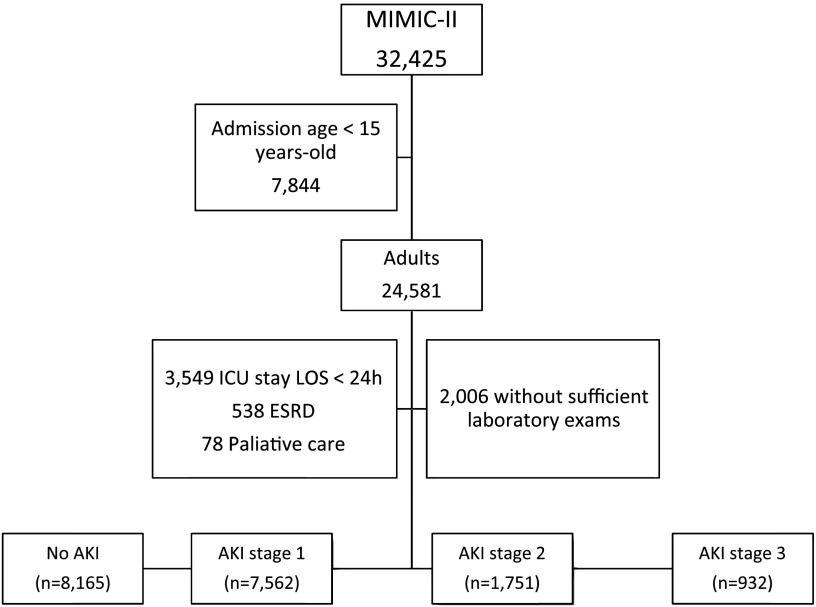
Design, setting, participants, & measurements: This was a retrospective analysis using data from the Multiparameter Intelligent Monitoring in Intensive Care II project. A total of 18,410 adult patients were enrolled from four intensive care units from a university hospital from 2001 to 2008.
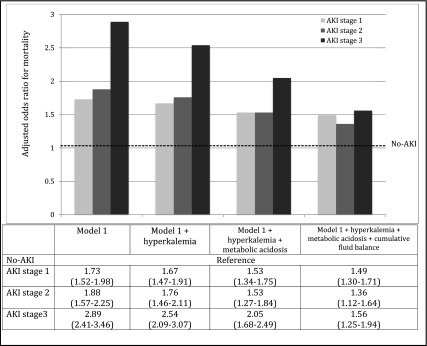
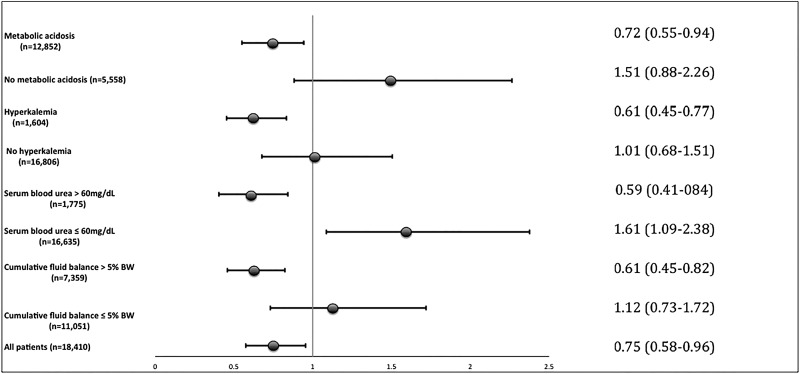
Results: Overall, 10,245 patients developed AKI. After adjustments, the odds ratios (ORs) for hospital mortality were 1.73 (95% confidence interval [95% CI], 1.52 to 1.98) for AKI stage 1, 1.88 (95% CI, 1.57 to 2.25) for stage 2, and 2.89 (95% CI, 2.41 to 3.46) for stage 3. Totals of 33%, 59%, and 70% of the excess mortality rates associated with AKI stages 1, 2, and 3, respectively, were attenuated by the inclusion of each AKI-related complication in the model. The main burden of excess hospital mortality associated with AKI was attenuated by metabolic acidosis and cumulative fluid balance. Long-term mortality was not attenuated by any of the associated complications. Next, we used two different approaches to explore the associations between RRT, AKI complications, and hospital mortality: multivariate analysis and propensity score matching. In both approaches, the sensitivity analysis for RRT was associated with a better hospital survival in only the following AKI-related subgroups: hyperkalemia (OR, 0.55; 95% CI, 0.35 to 0.85), metabolic acidosis (OR, 0.70; 95% CI, 0.53 to 0.92), cumulative fluid balance >5% of body weight (OR, 0.60; 95% CI, 0.40 to 0.88), and azotemia (OR, 0.57; 95% CI, 0.40 to 0.81).
Conclusions: A majority of the excess risk of mortality associated with AKI was attenuated by its fluid volume and metabolic complications, particularly in severe AKI. In addition, this study demonstrated that RRT is associated with a better outcome in patients with AKI-related complications.
Keywords: ARF; hemodialysis; mortality.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Ali T, Khan I, Simpson W, Prescott G, Townend J, Smith W, Macleod A: Incidence and outcomes in acute kidney injury: A comprehensive population-based study. J Am Soc Nephrol 18: 1292–1298, 2007 - PubMed
-
- Waikar SS, Curhan GC, Wald R, McCarthy EP, Chertow GM: Declining mortality in patients with acute renal failure, 1988 to 2002. J Am Soc Nephrol 17: 1143–1150, 2006 - PubMed
-
- Thakar CV, Christianson A, Freyberg R, Almenoff P, Render ML: Incidence and outcomes of acute kidney injury in intensive care units: A Veterans Administration study. Crit Care Med 37: 2552–2558, 2009 - PubMed
-
- Uchino S, Bellomo R, Goldsmith D, Bates S, Ronco C: An assessment of the RIFLE criteria for acute renal failure in hospitalized patients. Crit Care Med 34: 1913–1917, 2006 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
