

Intradialytic hypotension and risk of cardiovascular disease
- PMID: 25376764
- PMCID: PMC4255399
- DOI: 10.2215/CJN.02680314
Intradialytic hypotension and risk of cardiovascular disease
Abstract
Background and objectives: Patients undergoing hemodialysis have an elevated risk of cardiovascular disease-related morbidity and mortality compared with the general population. Intradialytic hypotension (IDH) is estimated to occur during 20%-30% of hemodialysis sessions. To date, no large studies have examined whether IDH is associated with cardiovascular outcomes. This study determined the prevalence of IDH according to interdialytic weight gain (IDWG) and studied the association between IDH and outcomes for cardiovascular events and mortality to better understand its role.
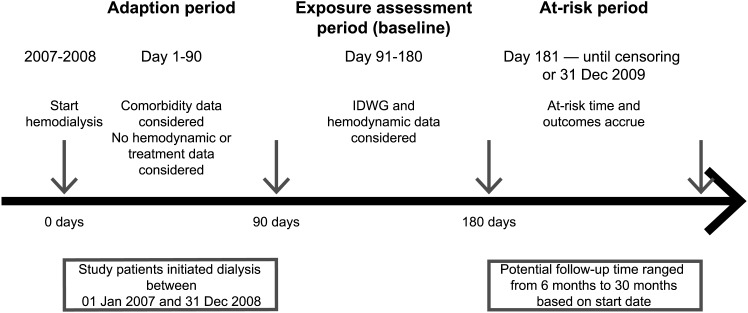
Design, setting, participants, & measurements: This study retrospectively examined records of 39,497 hemodialysis patients during 2007 and 2008. US Renal Data System claims and dialysis provider data were used to determine outcomes. IDH was defined by current Kidney Disease Outcomes Quality Initiative guidelines (≥20 mmHg fall in systolic BP from predialysis to nadir intradialytic levels plus ≥2 responsive measures [dialysis stopped, saline administered, etc.]). IDWG was measured absolutely (in kilograms) and relatively (in percentages).
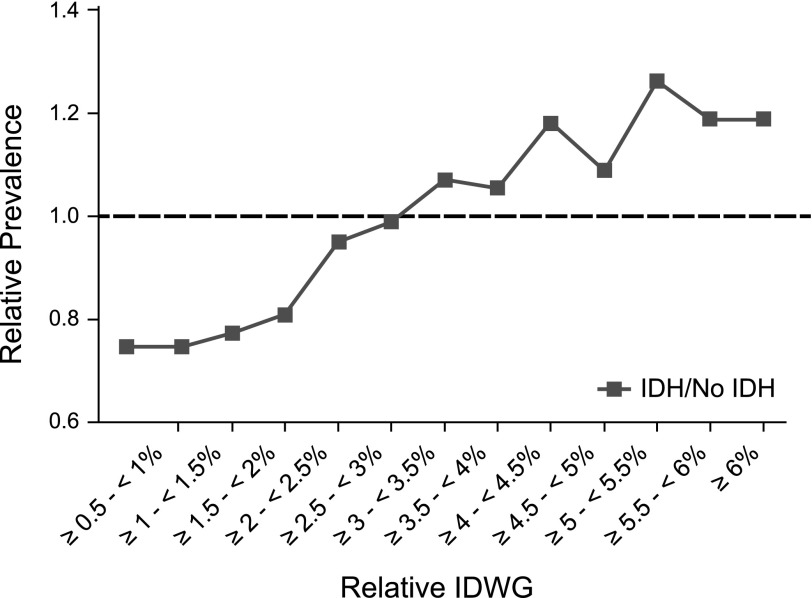
Results: IDH occurred in 31.1% of patients during the 90-day exposure assessment period. At baseline, the higher the IDWG (relative or absolute), the greater the frequency of IDH (P<0.001). For all-cause mortality, the median follow-up was 398 days (interquartile range, 231-602 days). Compared with patients without IDH, IDH was associated with all-cause mortality (7646 events; adjusted hazard ratio, 1.07 [95% confidence interval, 1.01 to 1.14]), myocardial infarction (2396 events; 1.20 [1.10 to 1.31]), hospitalization for heart failure/volume overload (8896 events; 1.13 [1.08 to 1.18]), composite hospitalization for heart failure/volume overload or cardiovascular mortality (10,805 events; 1.12 [1.08 to 1.17]), major adverse cardiac events (MACEs; myocardial infarction, stroke, cardiovascular mortality) (4994 events, 1.10 [1.03 to 1.17]), and MACEs+ (MACEs plus arrhythmia or hospitalization for heart failure/volume overload) (12,221 events; 1.14 [1.09 to 1.19]).
Conclusions: IDH was potently associated with cardiovascular morbidity and mortality. Clinical trials to ascertain causality are needed and should consider reduction in IDWG as a potential means to reduce IDH.
Keywords: ESRD; cardiovascular disease; hemodialysis; hypotension.
Copyright © 2014 by the American Society of Nephrology.
Figures
Comment in
-
Fluid management: the challenge of defining standards of care.Clin J Am Soc Nephrol. 2014 Dec 5;9(12):2033-5. doi: 10.2215/CJN.10341014. Epub 2014 Nov 6. Clin J Am Soc Nephrol. 2014. PMID: 25376766 Free PMC article. No abstract available.
References
-
- US Renal Data System: 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Available at http://www.usrds.org/atlas.aspx. Accessed October 10, 2013
-
- National Kidney Foundation: KDOQI Clinical Practice Guidelines for Cardiovascular Disease in Dialysis Patients. Available at http://www.kidney.org/professionals/kdoqi/guidelines_cvd/intradialytic.htm. Accessed October 16, 2013 - PubMed
-
- Palmer BF, Henrich WL: Recent advances in the prevention and management of intradialytic hypotension. J Am Soc Nephrol 19: 8–11, 2008 - PubMed
-
- Leypoldt JK, Cheung AK, Delmez JA, Gassman JJ, Levin NW, Lewis JA, Lewis JL, Rocco MV: Relationship between volume status and blood pressure during chronic hemodialysis. Kidney Int 61: 266–275, 2002 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
