

Open challenges in magnetic drug targeting
- PMID: 25377422
- PMCID: PMC4397114
- DOI: 10.1002/wnan.1311
Open challenges in magnetic drug targeting
Abstract
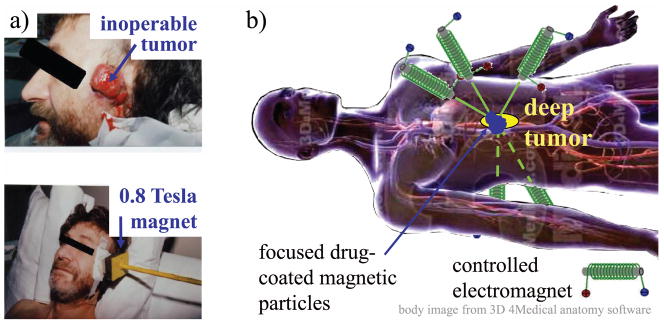
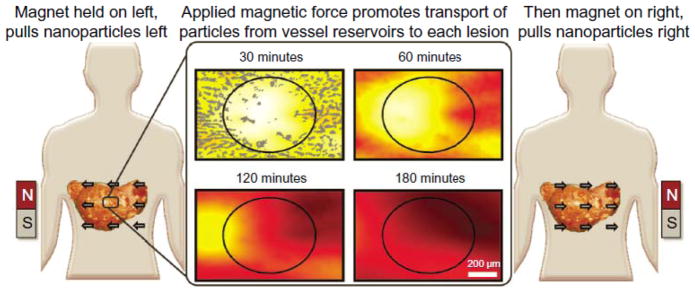
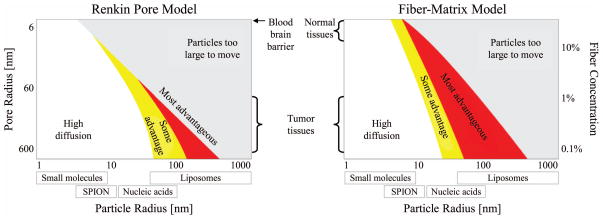
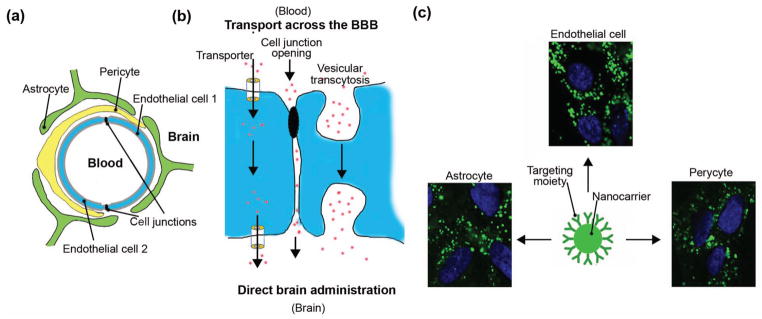
The principle of magnetic drug targeting, wherein therapy is attached to magnetically responsive carriers and magnetic fields are used to direct that therapy to disease locations, has been around for nearly two decades. Yet our ability to safely and effectively direct therapy to where it needs to go, for instance to deep tissue targets, remains limited. To date, magnetic targeting methods have not yet passed regulatory approval or reached clinical use. Below we outline key challenges to magnetic targeting, which include designing and selecting magnetic carriers for specific clinical indications, safely and effectively reaching targets behind tissue and anatomical barriers, real-time carrier imaging, and magnet design and control for deep and precise targeting. Addressing these challenges will require interactions across disciplines. Nanofabricators and chemists should work with biologists, mathematicians, and engineers to better understand how carriers move through live tissues and how to optimize carrier and magnet designs to better direct therapy to disease targets. Clinicians should be involved early on and throughout the whole process to ensure the methods that are being developed meet a compelling clinical need and will be practical in a clinical setting. Our hope is that highlighting these challenges will help researchers translate magnetic drug targeting from a novel concept to a clinically available treatment that can put therapy where it needs to go in human patients.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Lubbe AS, Bergemann C, Riess H, Schriever F, Reichardt P, et al. Clinical experiences with magnetic drug targeting: a phase i study with 4′-epidoxorubicin in 14 patients with advanced solid tumors. Cancer Research. 1996;56(20):4686–93. - PubMed
-
- Lemke AJ, von Pilsach MIS, Lubbe A, Bergemann C, Riess H, Felix R. Mri after magnetic drug targeting in patients with advanced solid malignant tumors. European Radiology. 2004;14(11):1949–55. - PubMed
-
- Voltairas PA, Fotiadis DI, Michalis LK. Hydrodynamics of magnetic drug targeting. Journal of Biomechanics. 2002;35(6):813–21. - PubMed
-
- Grief AD, Richardson G. Mathematical modeling of magnetically targeted drug delivery. Journal of Magnetism and Magnetic Materials - Proceedings of the Fifth International Conference on Scientific and Clinical Applications of Magnetic Carriers. 2005;293(1):455–63.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
