

Loss to follow-up in the Australian HIV Observational Database
- PMID: 25377928
- PMCID: PMC4424189
- DOI: 10.3851/IMP2916
Loss to follow-up in the Australian HIV Observational Database
Abstract
Background: Loss to follow-up (LTFU) in HIV-positive cohorts is an important surrogate for interrupted clinical care, which can potentially influence the assessment of HIV disease status and outcomes. After preliminary evaluation of LTFU rates and patient characteristics, we evaluated the risk of mortality by LTFU status in a high-resource setting.
Methods: Rates of LTFU were measured in the Australian HIV Observational Database for a range of patient characteristics. Multivariate repeated measures regression methods were used to identify determinants of LTFU. Mortality by LTFU status was ascertained using linkage to the National Death Index. Survival following combination antiretroviral therapy initiation was investigated using the Kaplan-Meier (KM) method and Cox proportional hazards models.
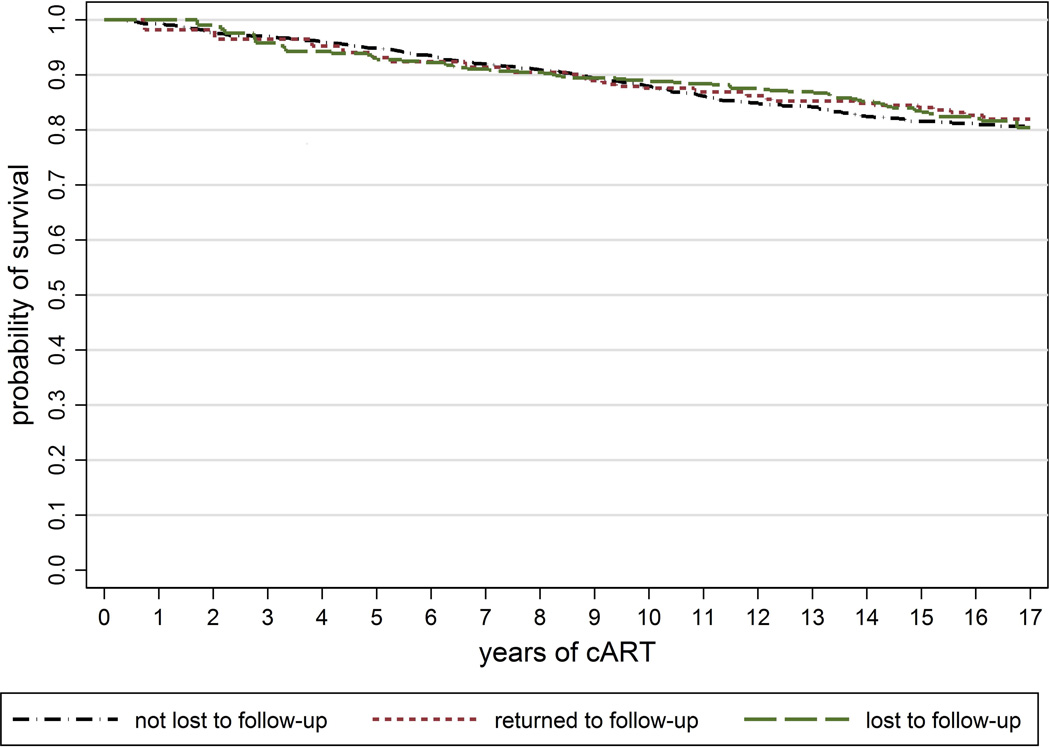
Results: Of 3,413 patients included in this analysis, 1,632 (47.8%) had at least one episode of LTFU after enrolment. Multivariate predictors of LTFU included viral load (VL)>10,000 copies/ml (rate ratio [RR] 1.63; 95% CI 1.45, 1.84; ref ≤400), time under follow-up (per year; RR 1.03; 95% CI 1.02, 1.04) and prior LTFU (per episode; RR 1.15; 95% CI 1.06, 1.24). KM curves for survival were similar by LTFU status (P=0.484). LTFU was not associated with mortality in Cox proportional hazards models (univariate hazard ratio [HR] 0.93; 95% CI 0.69, 1.26) and multivariate HR 1.04 (95% CI 0.77, 1.43).
Conclusions: Increased risk of LTFU was identified amongst patients with potentially higher infectiousness. We did not find significant mortality risk associated with LTFU. This is consistent with timely re-engagement with treatment, possibly via high levels of unreported linkage to other health-care providers.
References
-
- Dalal RP, Macphail C, Mqhayi M, Wing J, Feldman C, Chersich MF, et al. Characteristics and outcomes of adult patients lost to follow-up at an antiretroviral treatment clinic in johannesburg, South Africa. J Acquir Immune Defic Syndr. 2008;47(1):101–107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
