

The development of auditory perception in children after auditory brainstem implantation
- PMID: 25377987
- PMCID: PMC4289463
- DOI: 10.1159/000363684
The development of auditory perception in children after auditory brainstem implantation
Abstract
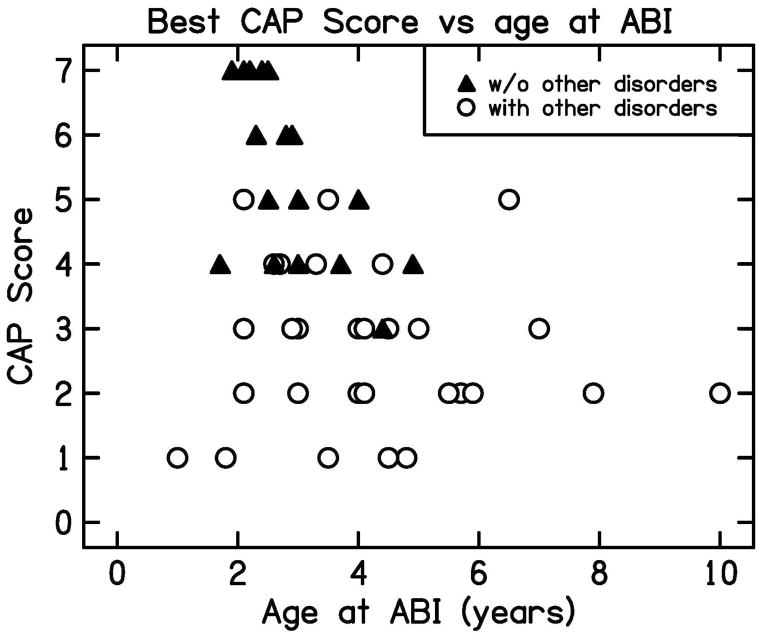
Auditory brainstem implants (ABIs) can provide useful auditory perception and language development in deaf children who are not able to use a cochlear implant (CI). We prospectively followed up a consecutive group of 64 deaf children up to 12 years following ABI surgery. The etiology of deafness in these children was: cochlear nerve aplasia in 49, auditory neuropathy in 1, cochlear malformations in 8, bilateral cochlear postmeningitic ossification in 3, neurofibromatosis type 2 in 2, and bilateral cochlear fractures due to a head injury in 1. Thirty-five children had other congenital nonauditory disabilities. Twenty-two children had previous CIs with no benefit. Fifty-eight children were fitted with the Cochlear 24 ABI device and 6 with the MedEl ABI device, and all children followed the same rehabilitation program. Auditory perceptual abilities were evaluated on the Categories of Auditory Performance (CAP) scale. No child was lost to follow-up, and there were no exclusions from the study. All children showed significant improvement in auditory perception with implant experience. Seven children (11%) were able to achieve the highest score on the CAP test; they were able to converse on the telephone within 3 years of implantation. Twenty children (31.3%) achieved open set speech recognition (CAP score of 5 or greater) and 30 (46.9%) achieved a CAP level of 4 or greater. Of the 29 children without nonauditory disabilities, 18 (62%) achieved a CAP score of 5 or greater with the ABI. All children showed continued improvements in auditory skills over time. The long-term results of ABI surgery reveal significant auditory benefit in most children, and open set auditory recognition in many.
© 2014 S. Karger AG, Basel.
Figures



References
-
- Archbold SM, Lutman E, Marshall D. Categories of Auditory Performance. Ann Otol Rhinol Laryngol. 1995;104 (Suppl 166):312–314. - PubMed
-
- Archbold SM, Lutman E, Nikolopoulos T. Categories of auditory performance: inter-user reliability. Br J Audiol. 1998;32:7–12. - PubMed
-
- Buchman CA, Teagle HF, Roush PA, Park LR, Hatch D, Woodard J, Zdanski C, Adunka OF. Cochlear implantation in children with labyrinthine anomalies and cochlear nerve deficiency: implications for auditory brainstem implantation. Laryngoscope. 2011;121(9):1979–88. - PubMed
-
- Carner M, Colletti V, Shannon R, Cerini R, Barillari M, Colletti L. Imaging in 28 Children with Cochlear Nerve Aplasia. Acta Otolaryngologica. 2009;129(4):458–61. - PubMed
-
- Casselman J, Mermuys K, Delanote J, Ghekiere J, Coenegrachts K. MRI of the cranial nerves--more than meets the eye: technical considerations and advanced anatomy. Neuroimaging Clin N Am. 2008;18(2):197–231. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
