

Risk of preterm delivery with increasing depth of excision for cervical intraepithelial neoplasia in England: nested case-control study
- PMID: 25378384
- PMCID: PMC4220819
- DOI: 10.1136/bmj.g6223
Risk of preterm delivery with increasing depth of excision for cervical intraepithelial neoplasia in England: nested case-control study
Erratum in
- BMJ. 2014;349:g7406. Chin, S [corrected to China, S]
Abstract
Objective: To determine the association between depth of excision of cervical intraepithelial neoplasia and risk of preterm birth.
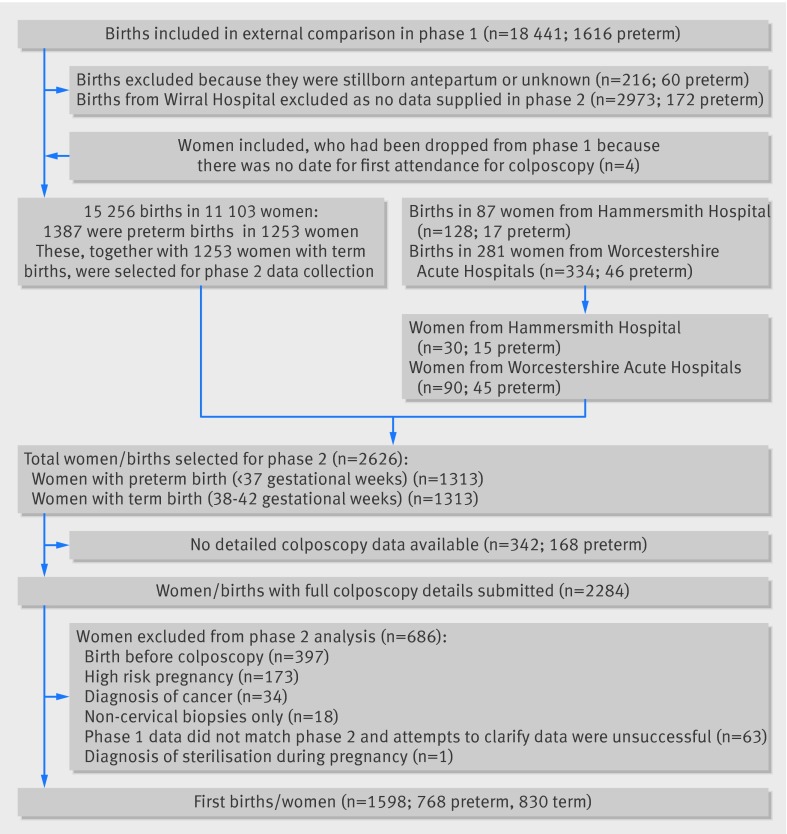
Design: Case-control study nested in record linkage cohort study.
Setting: 12 hospitals in England.
Participants: From a cohort of 11 471 women with at least one histological sample taken at colposcopy and a live singleton birth (before or after colposcopy), 1313 women with a preterm birth (20-36 weeks) were identified and frequency matched on maternal age at delivery, parity, and study site to 1313 women with term births (38-42 weeks).
Main outcome measures: Risk of preterm birth and very/extreme preterm birth by depth of excisional treatment of the cervical transformation zone.
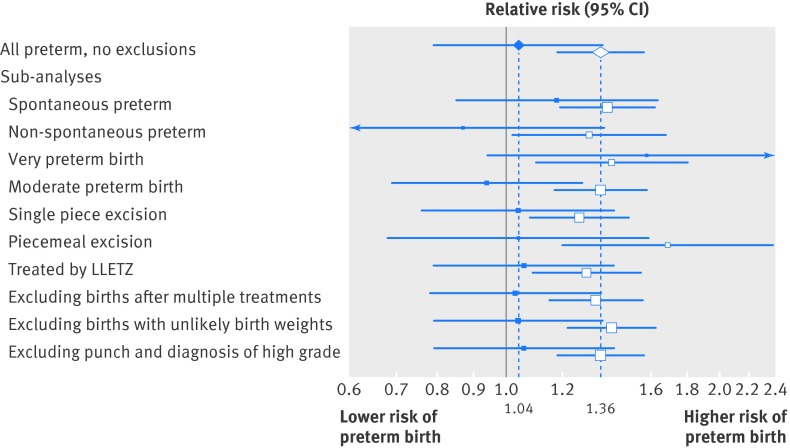
Results: After exclusions, 768 preterm births (cases) and 830 term births after colposcopy remained. The risk of preterm birth was no greater in women with a previous small (<10 mm) excision (absolute risk 7.5%, 95% confidence interval 6.0% to 8.9%) than in women with a diagnostic punch biopsy (7.2%, 5.9% to 8.5%). Women with a medium (10-14 mm) (absolute risk 9.6%; relative risk 1.28, 0.98 to 1.68), large (15-19 mm) (15.3%; 2.04, 1.41 to 2.96), or very large (≥ 20 mm) excision (18.0%; 2.40, 1.53 to 3.75) had a higher risk of preterm delivery than those with small excision. The same pattern was seen in 161 women with very/extremely preterm births (20-31 weeks) and with increasing volume excised. Most births were conceived more than three years after colposcopy, and the risk of preterm delivery did not seem to depend on time from excision to conception.
Conclusions: The risk of preterm birth is at most minimally affected by a small excision. Larger excisions, particularly over 15 mm or 2.66 cm(3), are associated with a doubling of the risk of both preterm and very preterm births. The risk does not decrease with increasing time from excision to conception. Efforts should be made to excise the entire lesion while preserving as much healthy cervical tissue as possible. Close obstetric monitoring is warranted for women who have large excisions of the cervical transformation zone.
© Castanon et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Safety of modern treatment for cervical pre-cancer.BMJ. 2014 Nov 5;349:g6611. doi: 10.1136/bmj.g6611. BMJ. 2014. PMID: 25378385 No abstract available.
References
-
- Bruinsma FJ, Quinn MA. The risk of preterm birth following treatment for precancerous changes in the cervix: a systematic review and meta-analysis. BJOG 2011;118:1031-41. - PubMed
-
- Kyrgiou M, Koliopoulos G, Martin-Hirsch PL, Arbyn M, Prendiville W, Paraskevaidis E. Obstetric outcome after conservative treatment for intraepithelial or early invasive cervical lesions: systematic review and meta-analysis. Lancet 2006;367:489-98. - PubMed
-
- Noehr B, Jensen A, Frederiksen K, Tabor A, Kjaer SK. Loop electrosurgical excision of the cervix and subsequent risk for spontaneous preterm delivery: a population-based study of singleton deliveries during a 9-year period. Am J Obstet Gynecol 2009;201:33.e1-6. - PubMed
-
- Noehr B, Jensen A, Frederiksen K, Tabor A, Kjaer SK. Depth of cervical cone removed by loop electrosurgical excision procedure and subsequent risk of spontaneous preterm delivery. Obstet Gynecol 2009;114:1232-8. - PubMed
-
- Sadler L, Saftlas A, Wang W, Exeter M, Whittaker J, McCowan L. Treatment for cervical intraepithelial neoplasia and risk of preterm delivery. JAMA 2004;291:2100-6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical