

The speed of ultraearly hematoma growth in acute intracerebral hemorrhage
- PMID: 25378675
- PMCID: PMC4277674
- DOI: 10.1212/WNL.0000000000001076
The speed of ultraearly hematoma growth in acute intracerebral hemorrhage
Abstract
Objective: The prognostic importance of the speed of early hematoma growth in acute intracerebral hemorrhage (ICH) has not been well established. We aimed to determine the association between the rate of increase in hematoma volume and major clinical outcomes in the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) studies. The effects of early intensive blood pressure (BP) lowering according to the speed of hematoma growth were also investigated.
Methods: Pooled analyses of the INTERACT1 (n = 404) and INTERACT2 (n = 2,839) studies-randomized controlled trials of patients with spontaneous ICH with elevated systolic BP, randomly assigned to intensive (target systolic BP <140 mm Hg) or guideline-based (<180 mm Hg) BP management. The speed of ultraearly hematoma growth (UHG) was defined as hematoma volume (mL)/onset-to-CT time (hours). Primary outcome was death or major disability (modified Rankin Scale score of 3-6) at 90 days.
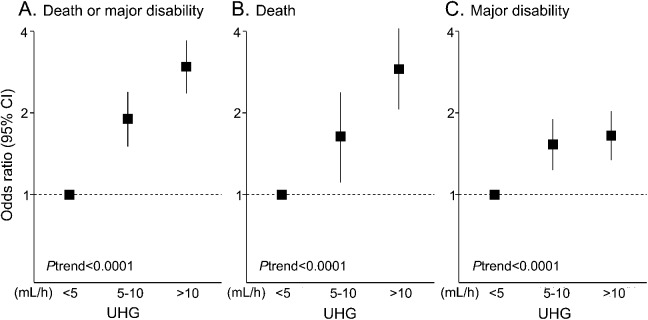
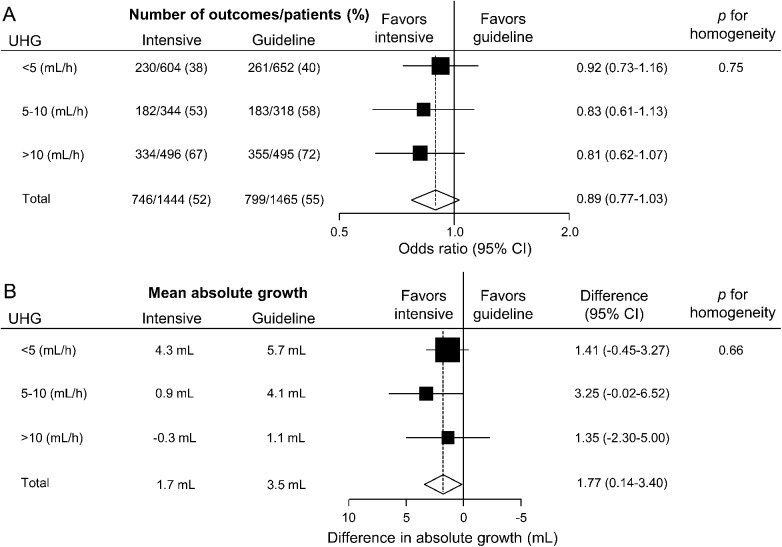
Results: Among a total of 2,909 patients (90%) with information on UHG and outcome, median speed of UHG was 6.2 mL/h. There was a linear association between UHG and outcome: multivariable-adjusted odd ratios 1.90 (95% confidence interval 1.50-2.39) for 5-10 mL/h and 2.96 (2.36-3.71) for >10 mL/h vs the <5 mL/h group. There were no clear differences in the effects of intensive BP lowering according to 3 speeds of UHG on outcome (p = 0.75 for homogeneity).
Conclusions: The speed of UHG in patients with ICH was continuously associated with increased risks of death or major disability, and from lower levels than previously reported (≥5 mL/h). The benefits of intensive BP lowering appear to be independent of the speed of bleeding.
© 2014 American Academy of Neurology.
Figures
References
-
- Rodriguez-Luna D, Rubiera M, Ribo M, et al. Ultraearly hematoma growth predicts poor outcome after acute intracerebral hemorrhage. Neurology 2011;77:1599–1604. - PubMed
-
- Anderson CS, Huang Y, Wang JG, et al. Intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT): a randomised pilot trial. Lancet Neurol 2008;7:391–399. - PubMed
-
- Delcourt C, Huang Y, Wang J, et al. The second (main) phase of an open, randomised, multicentre study to investigate the effectiveness of an intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT2). Int J Stroke 2010;5:110–116. - PubMed
-
- Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med 2013;368:2355–2365. - PubMed
-
- Marti-Fabregas J, Delgado-Mederos R, Granell E, et al. Microbleed burden and hematoma expansion in acute intracerebral hemorrhage. Eur Neurol 2013;70:175–178. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources