

Resting state connectivity correlates with drug and placebo response in fibromyalgia patients
- PMID: 25379438
- PMCID: PMC4215460
- DOI: 10.1016/j.nicl.2014.09.007
Resting state connectivity correlates with drug and placebo response in fibromyalgia patients
Abstract
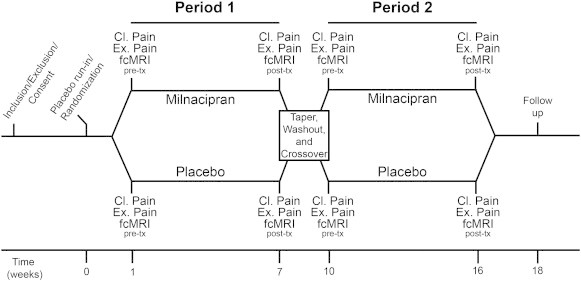
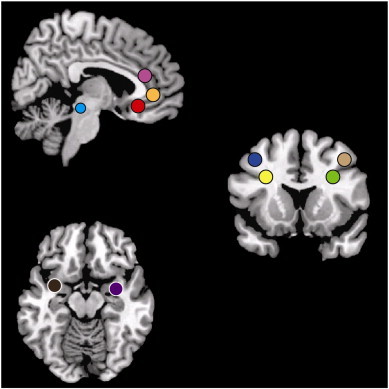
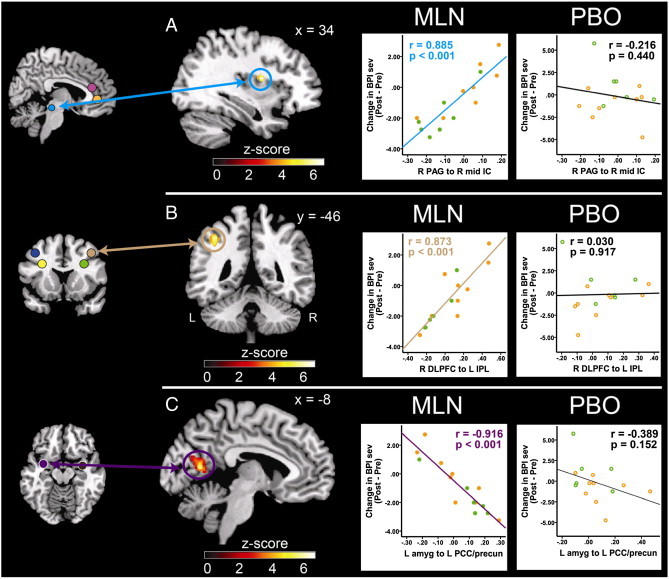
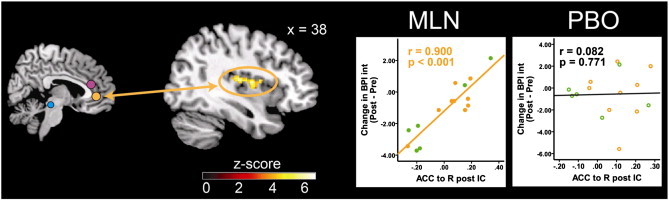
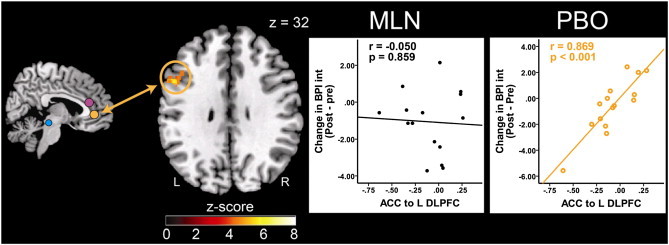
Fibromyalgia is a chronic pain syndrome characterized by widespread pain, fatigue, and memory and mood disturbances. Despite advances in our understanding of the underlying pathophysiology, treatment is often challenging. New research indicates that changes in functional connectivity between brain regions, as can be measured by magnetic resonance imaging (fcMRI) of the resting state, may underlie the pathogenesis of this and other chronic pain states. As such, this parameter may be able to be used to monitor changes in brain function associated with pharmacological treatment, and might also be able to predict treatment response. We performed a resting state fcMRI trial using a randomized, placebo-controlled, cross-over design to investigate mechanisms of action of milnacipran (MLN), a selective serotonin and norepinephrine reuptake inhibitor (SNRI), in fibromyalgia patients. Our aim was to identify functional connectivity patterns at baseline that would differentially predict treatment response to MLN as compared to placebo. Since preclinical studies of MLN suggest that this medication works by augmenting antinociceptive processes, we specifically investigated brain regions known to be involved in pain inhibition. 15 fibromyalgia patients completed the study, consisting of 6 weeks of drug and placebo intake (order counterbalanced) with an interspersed 2 week wash out period. As a main finding we report that reductions in clinical pain scores during MLN were associated with decreased functional connectivity between pro-nociceptive regions and antinociceptive pain regions at baseline, specifically between the rostral part of the anterior cingulate cortex (ACC) and the insular cortex (IC), as well as between the periaqueductal gray (PAG) and the IC: patients with lower preexisting functional connectivity had the greatest reduction in clinical pain. This pattern was not observed for the placebo period. However a more robust placebo response was associated with lower baseline functional connectivity between the ACC and the dorsolateral prefrontal cortex. This study indicates that ACC-IC connectivity might play a role in the mechanism of action of MLN, and perhaps more importantly fcMRI might be a useful tool to predict pharmacological treatment response.
Keywords: 5-HT, serotonin; ACC, anterior cingulate cortex; BPI, brief pain inventory; CNS, central nervous system; Chronic pain; DLPFC, dorsolateral prefrontal cortex; DMN, default mode network; FEW, family wise error; Fibromyalgia; Functional connectivity; IC, insular cortex; IPL, inferior parietal lobule; MCC, mid-cingulate cortex; MLN, milnacipran; NE, norepinephrine; PAG, periaqueductal gray; PCC, posterior cingulate cortex; QST, quantitative sensory testing; SNRI; SNRI, selective serotonin and norepinephrine reuptake inhibitor; SPM, statistical parametric mapping; TMS, transcranial magnetic stimulation; fMRI; fMRI, functional magnetic resonance imaging; fcMRI, functional connectivity magnetic resonance imaging; rs-fc, resting state functional connectivity.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
