

Impact of different etiologies of bronchiectasis on the pulmonary function tests
- PMID: 25380609
- PMCID: PMC4435083
- DOI: 10.3121/cmr.2014.1236
Impact of different etiologies of bronchiectasis on the pulmonary function tests
Abstract
Background: Bronchiectasis develops along the natural course of several respiratory and systemic conditions and induces significant changes in the morphofunctional structure of airways. Our objective was to assess the impact of various causes of bronchiectasis on clinical data, pulmonary function tests, and high-resolution computed tomography (HRCT).
Methods: The present report was a cross-sectional study that was conducted with 112 consecutive patients with bronchiectasis, who were allocated to five groups, as follows: sequelae of tuberculosis, history of non-tuberculosis infection, cystic fibrosis (CF), primary ciliary dyskinesia (PCD), and rheumatoid arthritis. All of the participants underwent spirometry, whole-body plethysmography, measurement of the diffusing capacity for carbon monoxide (DLco), and HRCT.
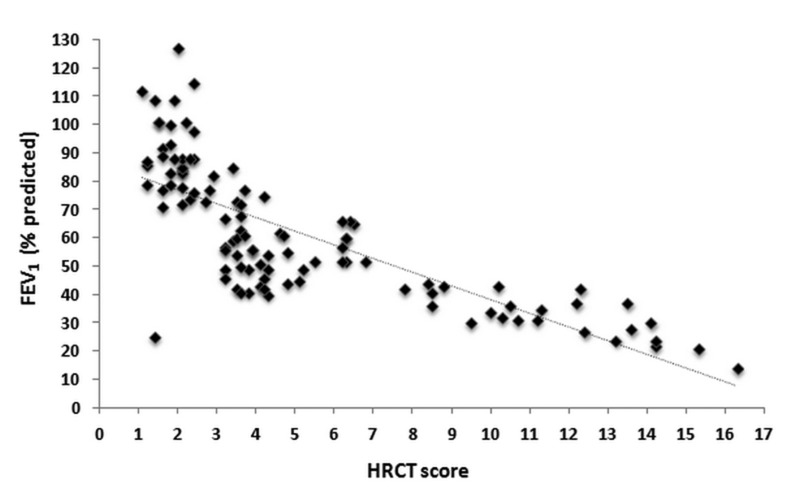
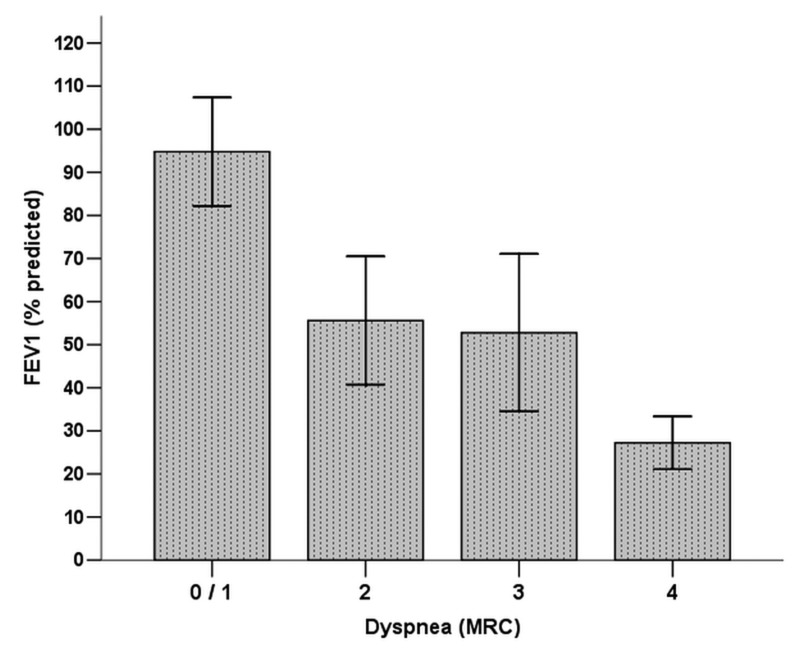
Results: The highest HRCT score was exhibited in patients with CF (6.03 ± 1.03). The values of forced expiratory volume in 1 second (FEV1) (52.2 ± 17.7%) and DLco (74.1 ± 15.2%) were lower in patients with sequelae of tuberculosis. The increase in the residual volume was more accentuated in the patients with CF (193.5 ± 39.5%) and PCD (189 ± 36.4%). By the multivariate analysis, the cause of FEV1 and bronchiectasis, HRCT score, and degree of dyspnea behaved as independent predictors of DLco.
Conclusion: In individuals with bronchiectasis, the pulmonary function abnormalities are associated with the etiology of the underlying disease.
Keywords: Bronchiectasis; Respiratory function tests; Respiratory mechanics; Tomography.
© 2015 Marshfield Clinic.
Figures
References
-
- Goeminne P, Dupont L. Non-cystic fibrosis bronchiectasis: diagnosis and management in 21st century. Postgrad Med J 2010;86:493–501. - PubMed
-
- Pasteur MC, Bilton D, Hill AT; British Thoracic Society Bronchiectasis non-CF Guideline Group. British Thoracic Society guideline for non-CF bronchiectasis. Thorax 2010;65:1–58. - PubMed
-
- Tsang KW, Chan K, Ho P, Zheng L, Ooi GC, Ho JC, Lam W. Sputum elastase in steady-state bronchiectasis. Chest 2000;117:420–426. - PubMed
-
- Barker AF, Bardana EJ., Jr Bronchiectasis: update of an orphan disease. Am Rev Respir Dis 1988;137:969–978. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources