

A phase 1b/2 study of vosaroxin in combination with cytarabine in patients with relapsed or refractory acute myeloid leukemia
- PMID: 25381131
- PMCID: PMC4803139
- DOI: 10.3324/haematol.2014.114769
A phase 1b/2 study of vosaroxin in combination with cytarabine in patients with relapsed or refractory acute myeloid leukemia
Abstract
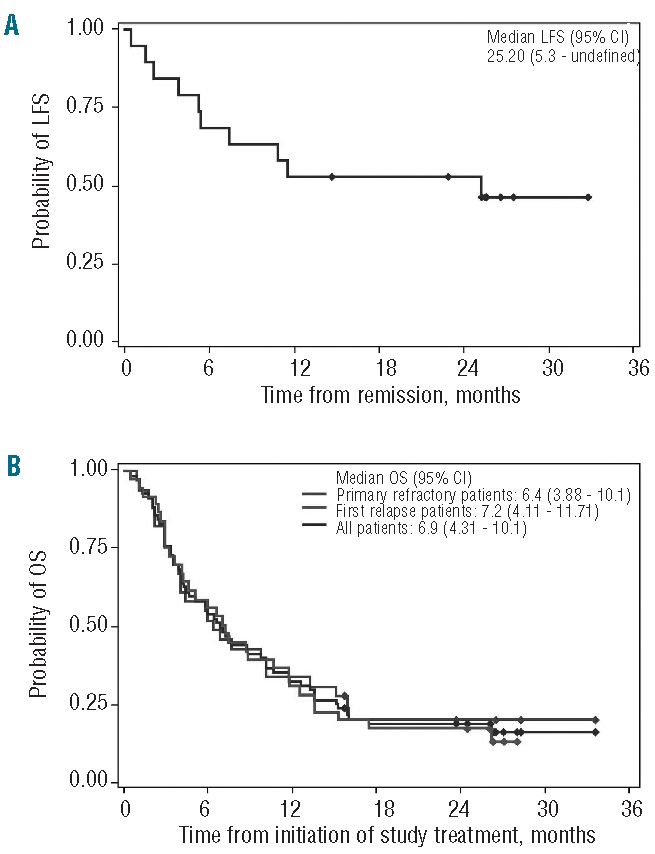
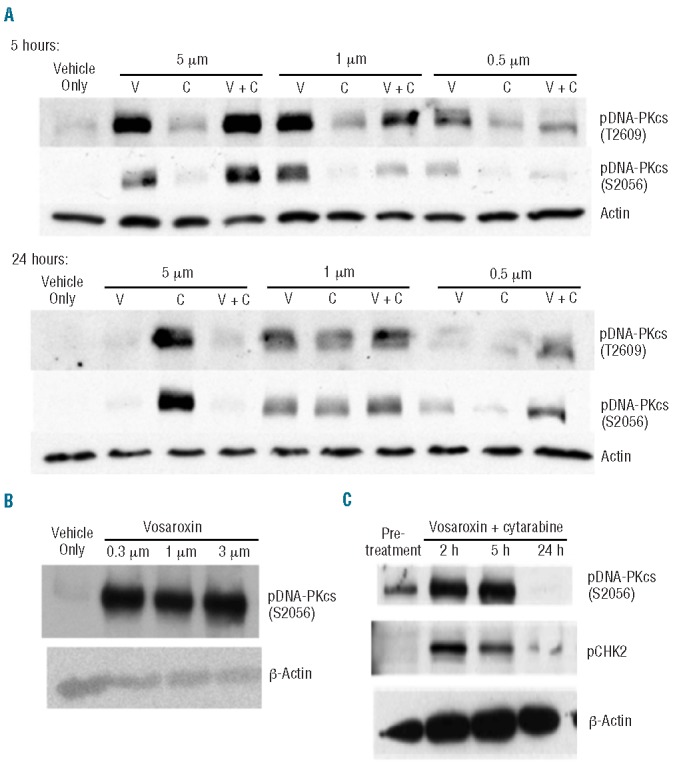
Vosaroxin is a first-in-class anticancer quinolone derivative that intercalates DNA and inhibits topoisomerase II. This study assessed the safety and tolerability of vosaroxin plus cytarabine in patients with relapsed/refractory acute myeloid leukemia. Escalating vosaroxin doses (10-minute infusion; 10-90 mg/m(2); days 1, 4) were given in combination with cytarabine on one of two schedules: schedule A (24-hour continuous intravenous infusion, 400 mg/m(2)/day, days 1-5) or schedule B (2-hour intravenous infusion, 1 g/m(2)/day, days 1-5). Following dose escalation, enrollment was expanded at the maximum tolerated dose. Of 110 patients enrolled, 108 received treatment. The maximum tolerated dose of vosaroxin was 80 mg/m(2) for schedule A (dose-limiting toxicities: grade 3 bowel obstruction and stomatitis) and was not reached for schedule B (recommended phase 2 dose: 90 mg/m(2)). In the efficacy population (all patients in first relapse or with primary refractory disease treated with vosaroxin 80-90 mg/m(2); n=69), the complete remission rate was 25% and the complete remission/complete remission with incomplete blood count recovery rate was 28%. The 30-day all-cause mortality rate was 2.5% among all patients treated at a dose of 80-90 mg/m(2). Based upon these results, a phase 3 trial of vosaroxin plus cytarabine was initiated in patients with relapsed/refractory acute myeloid leukemia. (Clinicaltrials.gov identifier: NCT00541866).
Copyright© Ferrata Storti Foundation.
Figures

References
-
- Breems DA, Van Putten WL, Huijgens PC, et al. Prognostic index for adult patients with acute myeloid leukemia in first relapse. J Clin Oncol. 2005;23(9):1969–1978. - PubMed
-
- Keating MJ, Kantarjian H, Smith TL, et al. Response to salvage therapy and survival after relapse in acute myelogenous leukemia. J Clin Oncol. 1989;7(8):1071–1080. - PubMed
-
- Leopold LH, Willemze R. The treatment of acute myeloid leukemia in first relapse: a comprehensive review of the literature. Leuk Lymphoma. 2002;43(9):1715–1727. - PubMed
-
- Lowenberg B, Downing JR, Burnett A. Acute myeloid leukemia. N Engl J Med. 1999;341(14):1051–1062. - PubMed
-
- Estey EH, Kantarjian HM. Therapy for acute myeloid leukemia. In: Hoffman R, Benz EJ, Jr, Shattil S, et al., eds. Hematology: Basic Principles and Practice. Philadelphia: Churchill Livingstone; 2004:1099–1120.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
