

Isolated endarteritis and kidney transplant survival: a multicenter collaborative study
- PMID: 25381427
- PMCID: PMC4413758
- DOI: 10.1681/ASN.2014020157
Isolated endarteritis and kidney transplant survival: a multicenter collaborative study
Abstract
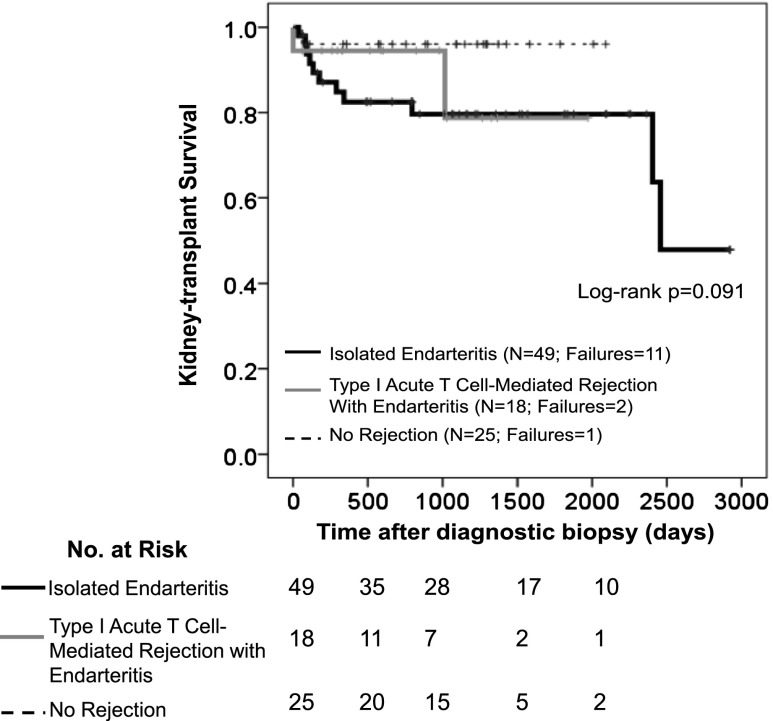
Isolated endarteritis of kidney transplants is increasingly recognized. Notably, microarray studies revealed absence of immunologic signatures of rejection in most isolated endarteritis biopsy samples. We investigated if isolated endarteritis responds to rejection treatment and affects kidney transplant survival. We retrospectively enrolled recipients of kidney transplant who underwent biopsies between 1999 and 2011 at seven American and Canadian centers. Exclusion criteria were recipients were blood group-incompatible or crossmatch-positive or had C4d-positive biopsy samples. After biopsy confirmation, patients were divided into three groups: isolated endarteritis (n=103), positive controls (type I acute T cell-mediated rejection with endarteritis; n=101), and negative controls (no diagnostic rejection; n=103). Primary end points were improved kidney function after rejection treatment and transplant failure. Mean decrease in serum creatinine from biopsy to 1 month after rejection treatment was 132.6 µmol/L (95% confidence interval [95% CI], 78.7 to 186.5) in patients with isolated endarteritis, 96.4 µmol/L (95% CI, 48.6 to 143.2) in positive controls (P=0.32), and 18.6 µmol/L (95% CI, 1.8 to 35.4) in untreated negative controls (P<0.001). Functional improvement after rejection treatment occurred in 80% of patients with isolated endarteritis and 81% of positive controls (P=0.72). Over the median 3.2-year follow-up period, kidney transplant survival rates were 79% in patients with isolated endarteritis, 79% in positive controls, and 91% in negative controls (P=0.01). In multivariate analysis, isolated endarteritis was associated with an adjusted 3.51-fold (95% CI, 1.16 to 10.67; P=0.03) risk for transplant failure. These data indicate that isolated endarteritis is an independent risk factor for kidney transplant failure.
Keywords: acute allograft rejection; kidney; transplantation; vasculitis.
Copyright © 2015 by the American Society of Nephrology.
Figures





Comment in
-
Renal allograft rejection: pieces of the puzzle.J Am Soc Nephrol. 2015 May;26(5):1004-5. doi: 10.1681/ASN.2014090932. Epub 2014 Nov 7. J Am Soc Nephrol. 2015. PMID: 25381428 Free PMC article. No abstract available.
References
-
- US Renal Data System : USRDS 2013 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2013
-
- Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, Saran R, Wang AY, Yang CW: Chronic kidney disease: Global dimension and perspectives. Lancet 382: 260–272, 2013 - PubMed
-
- Gill JS, Tonelli M: Penny wise, pound foolish? Coverage limits on immunosuppression after kidney transplantation. N Engl J Med 366: 586–589, 2012 - PubMed
-
- El-Zoghby ZM, Stegall MD, Lager DJ, Kremers WK, Amer H, Gloor JM, Cosio FG: Identifying specific causes of kidney allograft loss. Am J Transplant 9: 527–535, 2009 - PubMed
-
- Sellarés J, de Freitas DG, Mengel M, Reeve J, Einecke G, Sis B, Hidalgo LG, Famulski K, Matas A, Halloran PF: Understanding the causes of kidney transplant failure: The dominant role of antibody-mediated rejection and nonadherence. Am J Transplant 12: 388–399, 2012 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
