

Rituximab versus cyclophosphamide for ANCA-associated vasculitis with renal involvement
- PMID: 25381429
- PMCID: PMC4378104
- DOI: 10.1681/ASN.2014010046
Rituximab versus cyclophosphamide for ANCA-associated vasculitis with renal involvement
Abstract
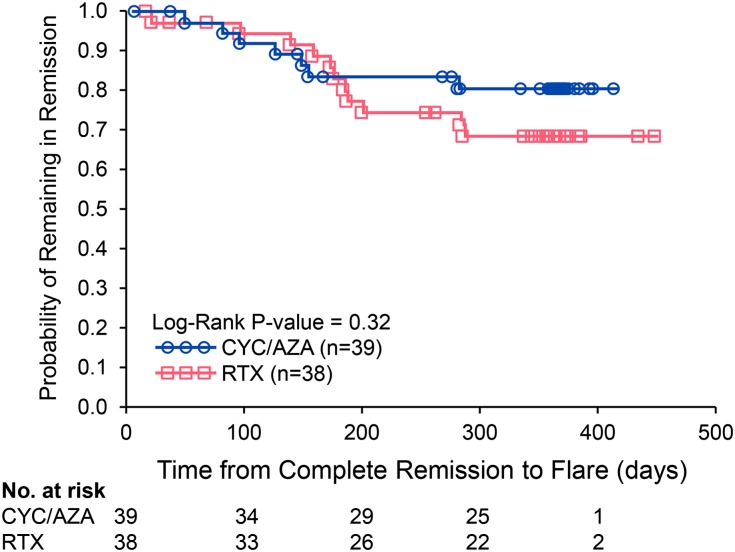
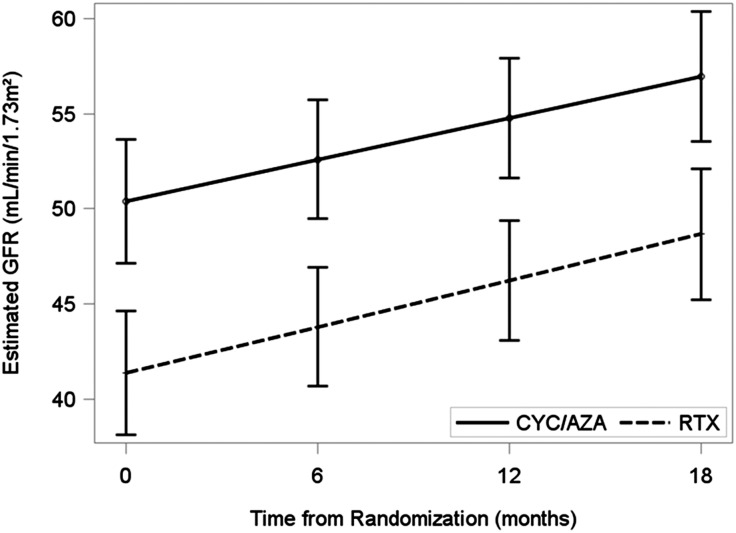
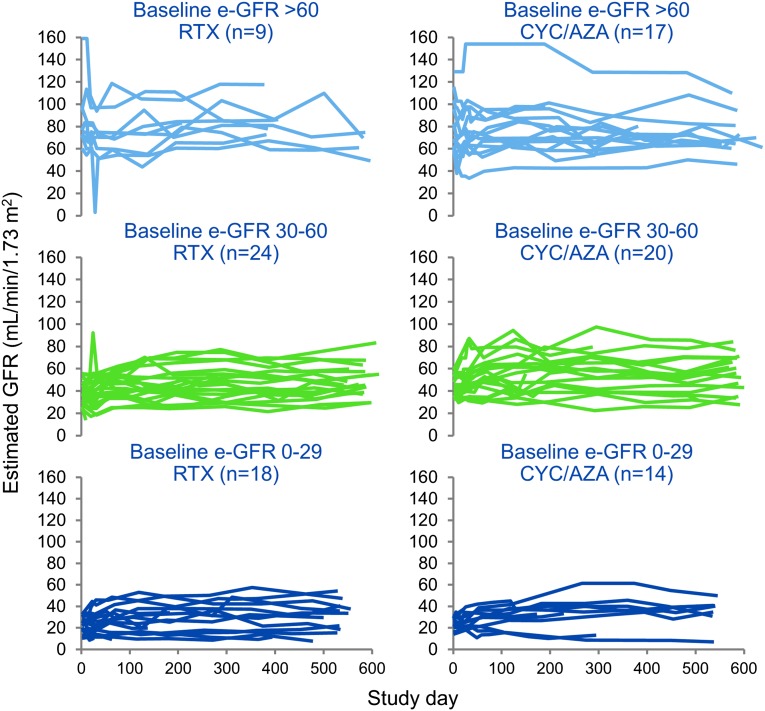
Rituximab (RTX) is non-inferior to cyclophosphamide (CYC) followed by azathioprine (AZA) for remission-induction in severe ANCA-associated vasculitis (AAV), but renal outcomes are unknown. This is a post hoc analysis of patients enrolled in the Rituximab for ANCA-Associated Vasculitis (RAVE) Trial who had renal involvement (biopsy proven pauci-immune GN, red blood cell casts in the urine, and/or a rise in serum creatinine concentration attributed to vasculitis). Remission-induction regimens were RTX at 375 mg/m(2) × 4 or CYC at 2 mg/kg/d. CYC was replaced by AZA (2 mg/kg/d) after 3-6 months. Both groups received glucocorticoids. Complete remission (CR) was defined as Birmingham Vasculitis Activity Score/Wegener's Granulomatosis (BVAS/WG)=0 off prednisone. Fifty-two percent (102 of 197) of the patients had renal involvement at entry. Of these patients, 51 were randomized to RTX, and 51 to CYC/AZA. Mean eGFR was lower in the RTX group (41 versus 50 ml/min per 1.73 m(2); P=0.05); 61% and 75% of patients treated with RTX and 63% and 76% of patients treated with CYC/AZA achieved CR by 6 and 18 months, respectively. No differences in remission rates or increases in eGFR at 18 months were evident when analysis was stratified by ANCA type, AAV diagnosis (granulomatosis with polyangiitis versus microscopic polyangiitis), or new diagnosis (versus relapsing disease) at entry. There were no differences between treatment groups in relapses at 6, 12, or 18 months. No differences in adverse events were observed. In conclusion, patients with AAV and renal involvement respond similarly to remission induction with RTX plus glucocorticoids or CYC plus glucocorticoids.
Keywords: ANCA; GN; vasculitis.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Understanding the role of rituximab in ANCA GN: regressing toward the mean.J Am Soc Nephrol. 2015 Apr;26(4):771-4. doi: 10.1681/ASN.2014100997. Epub 2014 Nov 7. J Am Soc Nephrol. 2015. PMID: 25381425 Free PMC article. No abstract available.
References
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, Rottem M, Fauci AS: Wegener granulomatosis: An analysis of 158 patients. Ann Intern Med 116: 488–498, 1992 - PubMed
-
- Fauci AS, Haynes BF, Katz P, Wolff SM: Wegener’s granulomatosis: Prospective clinical and therapeutic experience with 85 patients for 21 years. Ann Intern Med 98: 76–85, 1983 - PubMed
-
- Nachman PH, Hogan SL, Jennette JC, Falk RJ: Treatment response and relapse in antineutrophil cytoplasmic autoantibody-associated microscopic polyangiitis and glomerulonephritis. J Am Soc Nephrol 7: 33–39, 1996 - PubMed
-
- Stone JH, Merkel PA, Spiera R, Seo P, Langford CA, Hoffman GS, Kallenberg CG, St. Clair EW, Turkiewicz A, Tchao NK, Webber L, Ding L, Sejismundo LP, Mieras K, Weitzenkamp D, Ikle D, Seyfert-Margolis V, Mueller M, Brunetta P, Allen NB, Fervenza FC, Geetha D, Keogh KA, Kissin EY, Monach PA, Peikert T, Stegeman C, Ytterberg SR, Specks U, RAVE-ITN Research Group : Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med 363: 221–232, 2010 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K24-AR02224/AR/NIAMS NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- N01 AI015416/AI/NIAID NIH HHS/United States
- K23 AR052820/AR/NIAMS NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- K24 AR002224/AR/NIAMS NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1-RR025005/RR/NCRR NIH HHS/United States
- K24-AR049185/AR/NIAMS NIH HHS/United States
- K24 AR049185/AR/NIAMS NIH HHS/United States
- UL1-RR025771/RR/NCRR NIH HHS/United States
- K23-AR052820/AR/NIAMS NIH HHS/United States
- M01-RR00533/RR/NCRR NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- UL1 RR024150/RR/NCRR NIH HHS/United States
- UL1-RR024150-01/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
