

Athletic pubalgia and associated rehabilitation
- PMID: 25383246
- PMCID: PMC4223287
Athletic pubalgia and associated rehabilitation
Abstract
Background: Evaluation and treatment of groin pain in athletes is challenging. The anatomy is complex, and multiple pathologies often coexist. Different pathologies may cause similar symptoms, and many systems can refer pain to the groin. Many athletes with groin pain have tried prolonged rest and various treatment regimens, and received differing opinions as to the cause of their pain. The rehabilitation specialist is often given a non-specific referral of "groin pain" or "sports hernia." The cause of pain could be as simple as the effects of an adductor strain, or as complex as athletic pubalgia or inguinal disruption. The term "sports hernia" is starting to be replaced with more specific terms that better describe the injury. Inguinal disruption is used to describe the syndromes related to the injury of the inguinal canal soft tissue environs ultimately causing the pain syndrome. The term athletic pubalgia is used to describe the disruption and/or separation of the more medial common aponeurosis from the pubis, usually with some degree of adductor tendon pathology.
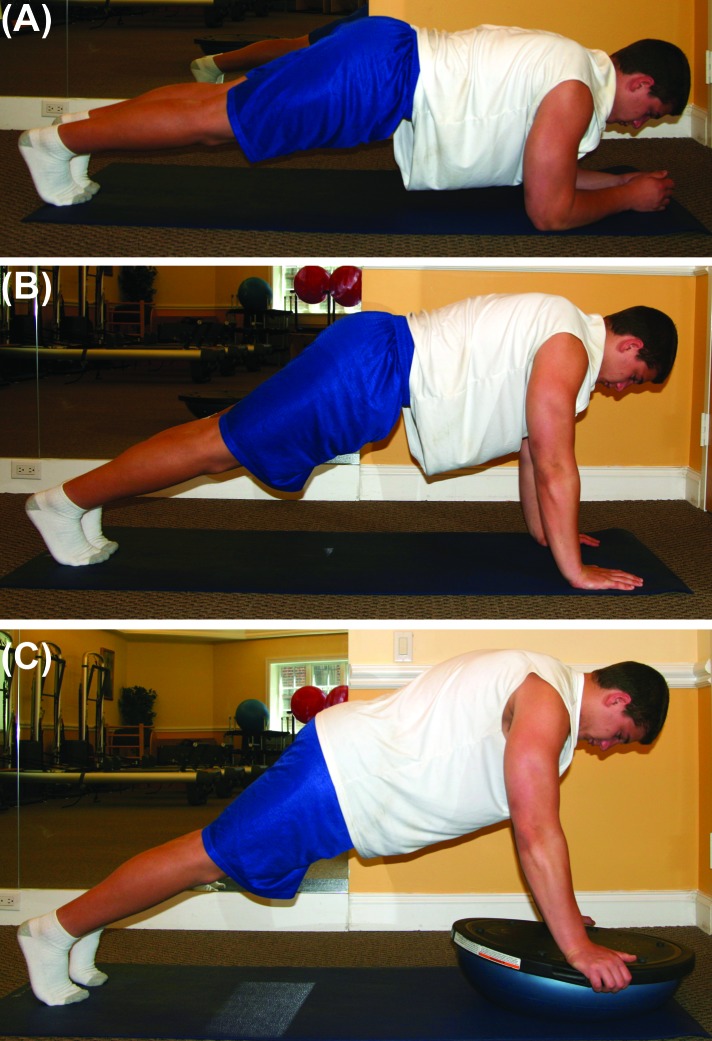
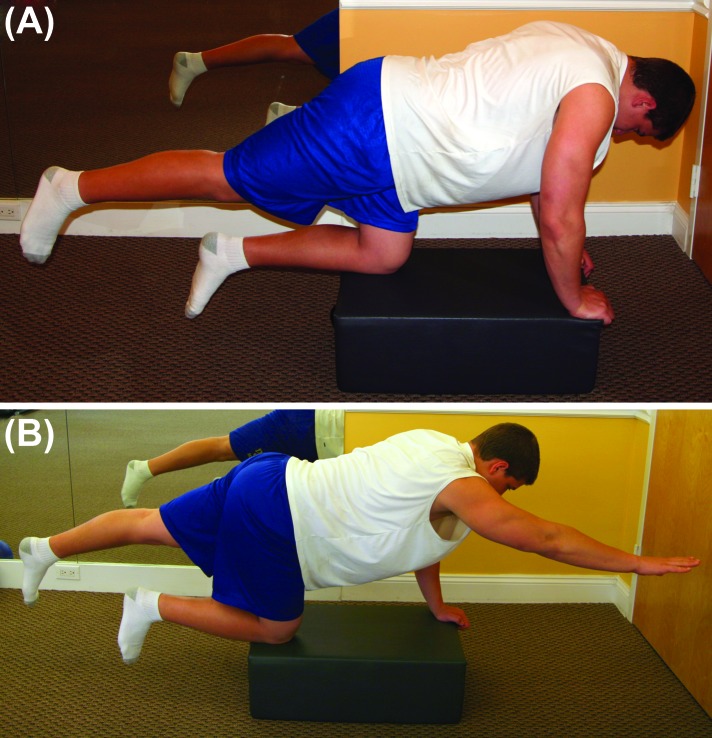
Treatment: Both non-operative and post-operative treatment options share the goal of returning the athlete back to pain free activity. There is little research available to reference for rehabilitation guidelines and creation of a plan of care. Although each surgeon has their own specific set of post-operative guidelines, some common concepts are consistent among most surgeons. Effective rehabilitation of the high level athlete to pain free return to play requires addressing the differences in the biomechanics of the dysfunction when comparing athletic pubalgia and inguinal disruption.
Conclusion: Proper evaluation and diagnostic skills for identifying and specifying the difference between athletic pubalgia and inguinal disruption allows for an excellent and efficient rehabilitative plan of care. Progression through the rehabilitative stages whether non-operative or post-operative allows for a focused rehabilitative program. As more information is obtained through MRI imaging and the diagnosis and treatment of inguinal disruption and athletic pubalgia becomes increasingly frequent, more research is warranted in this field to better improve the evidence based practice and rehabilitation of patients.
Levels of evidence: 5.
Keywords: Adductor strain; athletic pubalgia; groin pain; rehabilitation; sports hernia transversus abdominis.
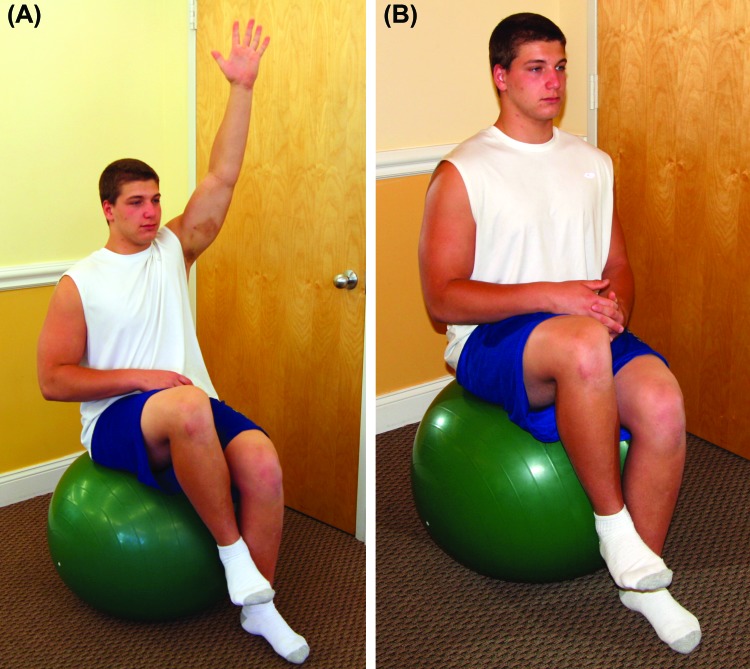
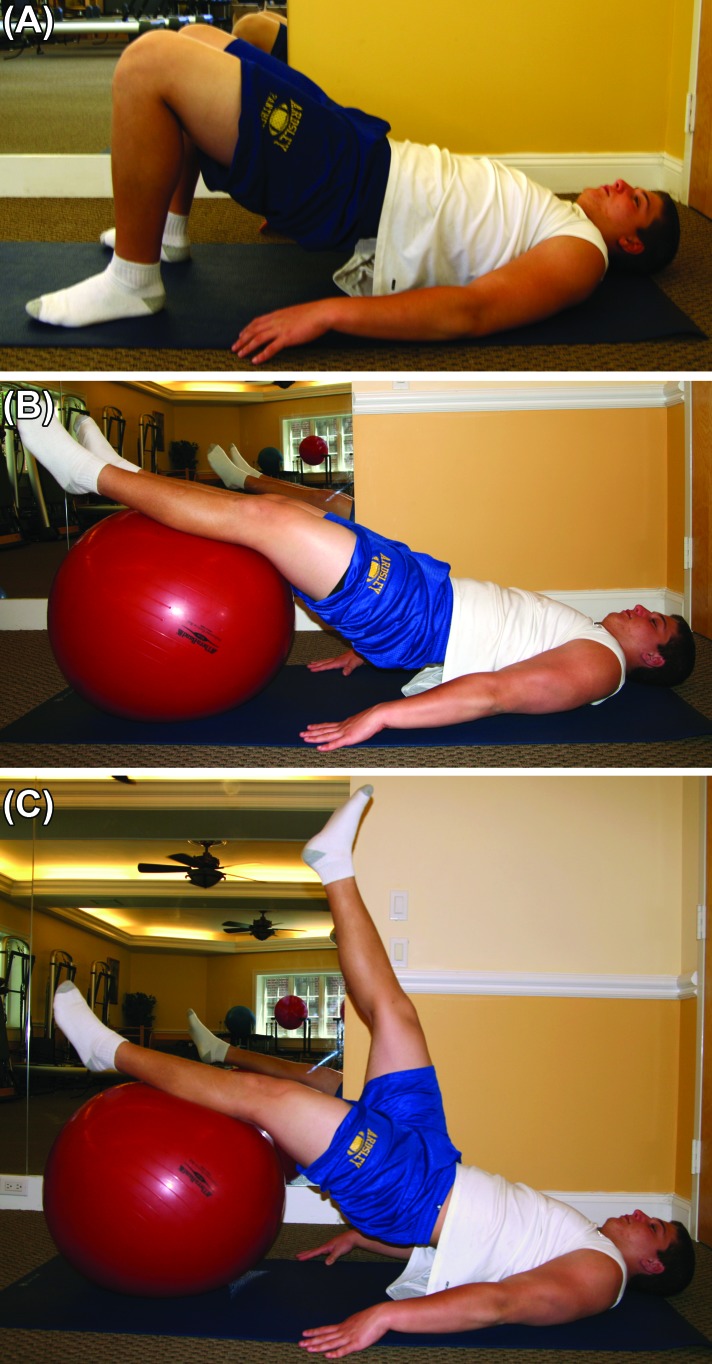
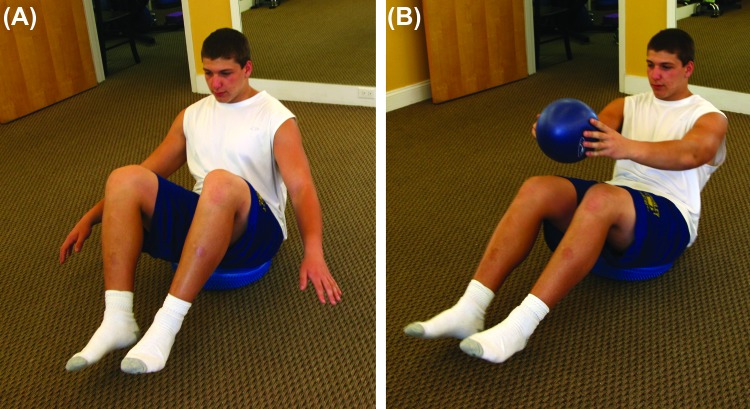
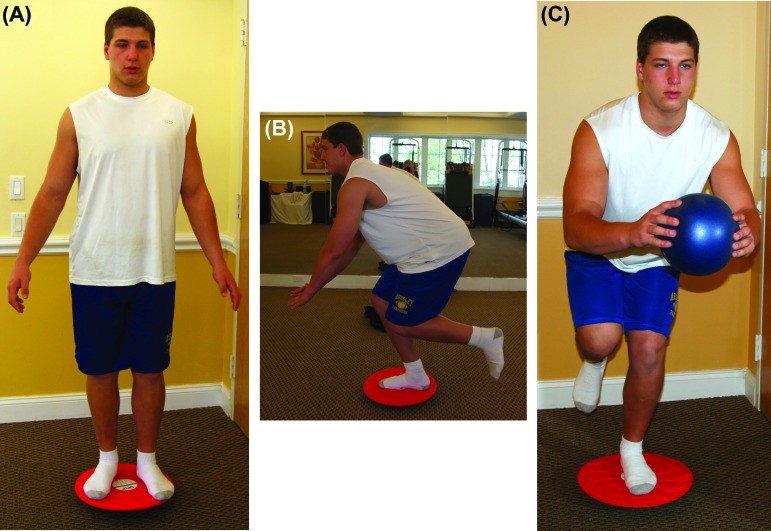
Figures



References
-
- Schilders E Dimitrakopouiou A Cooke M et al. Effectiveness of a selective partial release for chronic adductor‐related groin pain in professional athletes. Am J Sport Med. 2013;43:603‐607. - PubMed
-
- Minnich JM Hanks JB Muschaweck U et al. Sports Hernia: Diagnosis and treatment highlighting a minimal repair surgical technique. Am J Sport Med. 2013;39:1341‐1349. - PubMed
-
- Sheen AJ Stephenson BM Lloyd DM et al. Treatment of the Sportsman's groin: British Hernia Society's 2014 position statement based on the Manchester Consensus Conference. Br J Sports Med. 2013. 10.1136/bjsports-2013-092872. - PubMed
-
- Ahumada LA Ashruf S Espinosa‐de‐los‐Monteros A et al. Athletic pubalgia: Definition and surgical treatment. Ann Plast Surg. 2005;55(4):393‐396. - PubMed
-
- Joesting DR Diagnosis and treatment of sportsman's hernia. Curr Sports Med Rep. 2002;1(2):121‐124. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials