

Postoperative radiotherapy is associated with better survival in non-small cell lung cancer with involved N2 lymph nodes: results of an analysis of the National Cancer Data Base
- PMID: 25384064
- PMCID: PMC4336617
- DOI: 10.1097/JTO.0000000000000411
Postoperative radiotherapy is associated with better survival in non-small cell lung cancer with involved N2 lymph nodes: results of an analysis of the National Cancer Data Base
Abstract
Introduction: Use of postoperative radiotherapy (PORT) in non-small-cell lung cancer remains controversial. Limited data indicate that PORT may benefit patients with involved N2 nodes. This study evaluates this hypothesis in a large retrospective cohort treated with chemotherapy and contemporary radiation techniques.
Methods: The National Cancer Data Base was queried for patients diagnosed 2004-2006 with resected non-small-cell lung cancer and pathologically involved N2 (pN2) nodes also treated with chemotherapy. Multivariable Cox proportional hazards model was used to assess factors associated with overall survival (OS). Inverse probability of treatment weighting (IPTW) using the propensity score was used to reduce selection bias. OS was compared between patients treated with versus without PORT using the adjusted Kaplan-Meier estimator and weighted log-rank test based on IPTW.
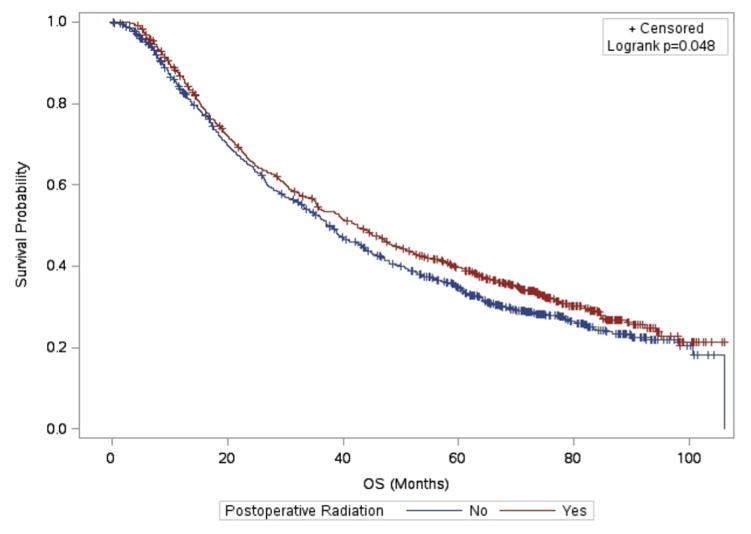
Results: Two thousand and one hundred and fifteen patients were eligible for analysis. 918 (43.4%) received PORT, 1197 (56.6%) did not. PORT was associated with better OS (median survival time 42 months with PORT versus 38 months without, p = 0.048). This effect was significant in multivariable and IPTW Cox models (hazard ratio: 0.87, 95% confidence interval: 0.78-0.98, p = 0.026, and hazard ratio: 0.89, 95% confidence interval: 0.79-1.00, p = 0.046, respectively). No interaction was seen between the effects of PORT and number of involved lymph nodes (p = 0.615).
Conclusions: PORT was associated with better survival for patients with pN2 nodes also treated with chemotherapy. No interaction was seen between benefit of PORT and number of involved nodes. These findings reinforce the benefit of PORT for N2 disease in modern practice using the largest, most recent cohort of chemotherapy-treated pN2 patients to date.
Conflict of interest statement
Conflicts of Interest: none
Figures

References
-
- Postoperative radiotherapy in non-small-cell lung cancer: systematic review and meta-analysis of individual patient data from nine randomised controlled trials. PORT Meta-analysis Trialists Group. Lancet. 1998 Jul 25;352(9124):257–263. - PubMed
-
- Bekelman JE, Rosenzweig KE, Bach PB, Schrag D. Trends in the use of postoperative radiotherapy for resected non-small-cell lung cancer. International journal of radiation oncology, biology, physics. 2006 Oct 1;66(2):492–499. - PubMed
-
- Munro AJ. What now for postoperative radiotherapy for lung cancer? Lancet. 1998 Jul 25;352(9124):250–251. - PubMed
-
- Phlips P, Rocmans P, Vanderhoeft P, Van Houtte P. Postoperative radiotherapy after pneumonectomy: impact of modern treatment facilities. International journal of radiation oncology, biology, physics. 1993 Oct 20;27(3):525–529. - PubMed
-
- Douillard JY, Rosell R, De Lena M, et al. Impact of postoperative radiation therapy on survival in patients with complete resection and stage I, II, or IIIA non-small-cell lung cancer treated with adjuvant chemotherapy: the adjuvant Navelbine International Trialist Association (ANITA) Randomized Trial. International journal of radiation oncology, biology, physics. 2008 Nov 1;72(3):695–701. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
