

Can combining femoral and acetabular morphology parameters improve the characterization of femoroacetabular impingement?
- PMID: 25384428
- PMCID: PMC4353537
- DOI: 10.1007/s11999-014-4037-4
Can combining femoral and acetabular morphology parameters improve the characterization of femoroacetabular impingement?
Abstract
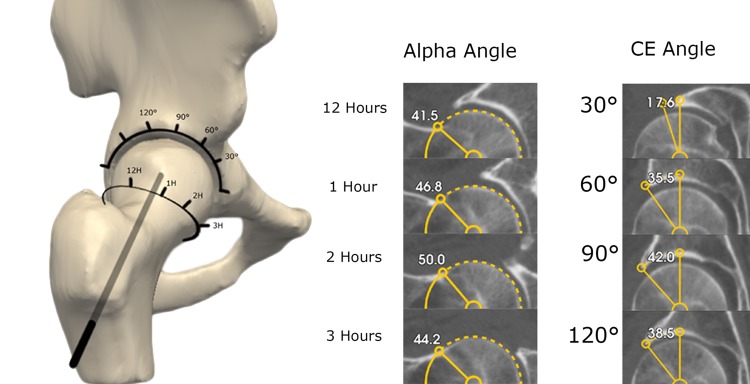
Background: Femoroacetabular impingement (FAI) presupposes a dynamic interaction of the proximal femur and acetabulum producing clinical symptoms and chondrolabral damage. Currently, FAI classification is based on alpha angle and center-edge angle measurements in a single plane. However, acetabular and femoral version and neck-shaft angle also influence FAI. Furthermore, each of these parameters has a reciprocal interaction with the others; for example, a shallow acetabulum delays impingement of the femoral head with the acetabular rim.
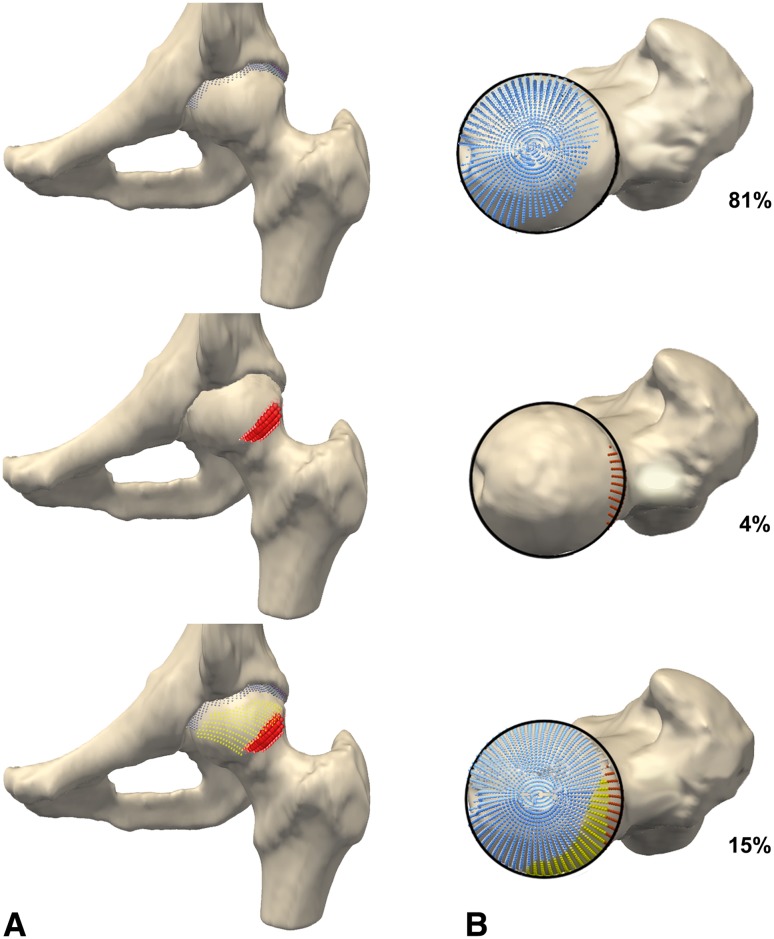
Questions/purposes: We introduce the new parameter "omega zone," which combines five parameters into one: the alpha and center-edge angles, acetabular and femoral version, and neck-shaft angle. We sought to determine whether the omega zone could differentiate patients with FAI from (1) normal control subjects (alpha < 55°), but also from (2) control subjects with elevated alpha angles (≥ 55°).
Methods: We evaluated CT data of 20 hips of male patients with symptomatic cam-type FAI and of 35 male hips extracted from 110 anonymized CT scans for vascular diagnosis. We excluded hips with osteoarthritis, developmental dysplasia, or coxa profunda (center-edge angle 20°-45° on AP pelvic view or corresponding coronal CT views). With dedicated software, femoral and pelvic orientation was standardized; we tested the omega zone in four hip positions in three distinct groups: patients with cam-type FAI (alpha > 60°) and control subjects with normal (< 55°) and high alpha angles (≥ 55°).
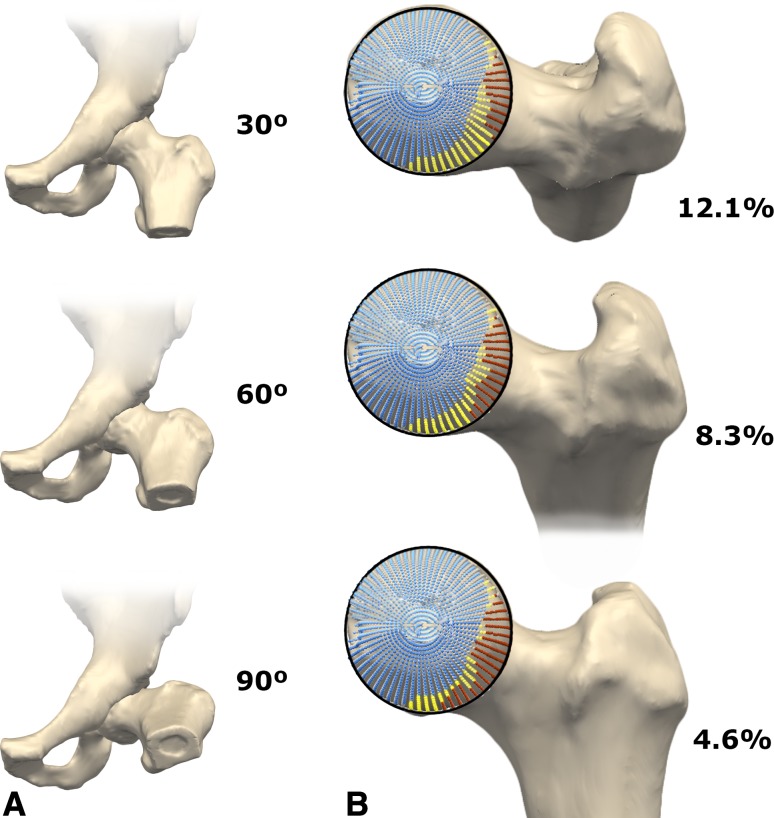
Results: The omega zone was smaller in patients with cam-type FAI than normal control subjects (alpha angle < 55°) at 60° and 90° of flexion (mean, 12%; 95% confidence interval [CI], 7-17; p = 0.008; Cohen's d = 9%; 95% CI, 4-13; p = 0.003). Furthermore, the omega zone was smaller in all positions in patients with cam-type FAI than control subjects with high alpha angles (0° p = 0.017, 30° p = 0.004, 60° p = 0.004, 90° p = 0.007). In contrast, the omega zone did not differ between control subjects with normal or high alpha angles. In all hips, the omega zone decreased with flexion, corresponding to a decrease in remaining impingement-free motion with flexion.
Conclusions: The omega zone visualizes and quantifies the interaction of the proximal femur and acetabulum. The omega zone differed between patients with cam-type FAI and control subjects with high alpha angles (≥ 55°), who could not be distinguished based on alpha angle alone. For hip-preserving surgery, it can help surgeons decide whether to address the femur, the acetabulum, or both.
Figures
References
-
- Agricola R, Reijman M, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH. Total hip replacement but not clinical osteoarthritis can be predicted by the shape of the hip: a prospective cohort study (CHECK) Osteoarthritis Cartilage. 2013;21:559–564. doi: 10.1016/j.joca.2013.01.005. - DOI - PubMed
-
- Arbabi E, Chegini S, Boulic R, Tannast M, Ferguson SJ, Thalmann D. Penetration depth method—novel real-time strategy for evaluating femoroacetabular impingement. J Orthop Res. 2010;28:880–886. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
